S-ar putea să vă placă și
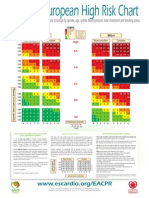
- 10 Year Risk of Fatal CVD in High Risk Regions of Europe by Gender, Age, Systolic Blood Pressure, Total Cholesterol and Smoking StatusDocument2 pagini10 Year Risk of Fatal CVD in High Risk Regions of Europe by Gender, Age, Systolic Blood Pressure, Total Cholesterol and Smoking StatusCotovici Catana AlinaÎncă nu există evaluări
- Algo Tachycardia PDFDocument1 paginăAlgo Tachycardia PDFYudhistira AdiÎncă nu există evaluări
- Intubation Techniques and ComplicationsDocument26 paginiIntubation Techniques and ComplicationsalexismutuyimanaÎncă nu există evaluări
- Post-Stroke Mood and Emotional Disturbances: Pharmacological Therapy Based On MechanismsDocument12 paginiPost-Stroke Mood and Emotional Disturbances: Pharmacological Therapy Based On MechanismsScribdMeUpÎncă nu există evaluări
- CtsDocument4 paginiCtsWindyÎncă nu există evaluări
- ScholarshipDocument1 paginăScholarshipWindyÎncă nu există evaluări
- 1Document6 pagini1WindyÎncă nu există evaluări
- High Consumption of Coffee Is Associated With Decreased Multiple Sclerosis Risk Results From Two Independent StudiesDocument8 paginiHigh Consumption of Coffee Is Associated With Decreased Multiple Sclerosis Risk Results From Two Independent StudiesWindyÎncă nu există evaluări
- E000083 FullDocument7 paginiE000083 FullWindyÎncă nu există evaluări
- Otitis MediaDocument84 paginiOtitis MediaAlex MatthewÎncă nu există evaluări
- Medical Terminology1Document41 paginiMedical Terminology1WindyÎncă nu există evaluări
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Epidemiology and Ethyology PneumoniaDocument11 paginiEpidemiology and Ethyology PneumoniaAnies DyaningÎncă nu există evaluări
- Anatomy - UPPER LIMB - 3 Muscles, Innervation and Compartments of The Upper LimbDocument20 paginiAnatomy - UPPER LIMB - 3 Muscles, Innervation and Compartments of The Upper LimbWindyÎncă nu există evaluări
- Idiopathic Thrombocytopenic Purpura (ITP) : Feature Disease FactsDocument3 paginiIdiopathic Thrombocytopenic Purpura (ITP) : Feature Disease Factsnisa_neyshaaljufriÎncă nu există evaluări
- Nocturia: ReviewDocument4 paginiNocturia: ReviewWindyÎncă nu există evaluări
- Widal TestDocument2 paginiWidal Testsarun5832Încă nu există evaluări
- Img 0001Document1 paginăImg 0001WindyÎncă nu există evaluări
- Diabetes InsipidusDocument7 paginiDiabetes Insipiduspaul_stefenson10Încă nu există evaluări
- DIabetes Care 2013Document114 paginiDIabetes Care 2013Jose Ricardo Castro ObesoÎncă nu există evaluări
- Biomedik 2Document9 paginiBiomedik 2Andi Rizki AyuÎncă nu există evaluări
- Widal TestDocument2 paginiWidal Testsarun5832Încă nu există evaluări
- What Are The Signs and Symptoms of Cushing'sDocument1 paginăWhat Are The Signs and Symptoms of Cushing'sWindyÎncă nu există evaluări
- Gerd ObesityDocument7 paginiGerd ObesityWindyÎncă nu există evaluări
- Aritmia 2-7-13 - 2Document58 paginiAritmia 2-7-13 - 2WindyÎncă nu există evaluări
- What Are The Signs and Symptoms of Cushing'sDocument1 paginăWhat Are The Signs and Symptoms of Cushing'sWindyÎncă nu există evaluări
- How to Optimize s for DocumentsDocument1 paginăHow to Optimize s for DocumentsWindyÎncă nu există evaluări
- Img 0001Document1 paginăImg 0001WindyÎncă nu există evaluări
- The Associated Press, Vancouver, British Colombia - Entertainment - Wed, July 17 2013, 10:31 AMDocument2 paginiThe Associated Press, Vancouver, British Colombia - Entertainment - Wed, July 17 2013, 10:31 AMWindyÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- WTRTFDocument384 paginiWTRTFNewsÎncă nu există evaluări
- Triage by Scott Anderson - Analytical EssayDocument5 paginiTriage by Scott Anderson - Analytical Essaygreensocks231Încă nu există evaluări
- Triage WorkbookDocument222 paginiTriage WorkbookYtamar Visbal Perez0% (1)
- Research Article: The Role Descriptions of Triage Nurse in Emergency Department: A Delphi StudyDocument6 paginiResearch Article: The Role Descriptions of Triage Nurse in Emergency Department: A Delphi StudyMathewos MekonnenÎncă nu există evaluări
- Unit One: a medical specialist who administers يطعي anesthetics نكسملا -ردخملا. heart surgeon, heart specialistDocument14 paginiUnit One: a medical specialist who administers يطعي anesthetics نكسملا -ردخملا. heart surgeon, heart specialistاحمد ابو زيدÎncă nu există evaluări
- Final Research Bulletin 2014 HEMOGLOBIN WHODocument483 paginiFinal Research Bulletin 2014 HEMOGLOBIN WHOnurul_sharaswatiÎncă nu există evaluări
- Emergency Rescue and TransferDocument35 paginiEmergency Rescue and Transferlura castroÎncă nu există evaluări
- Prehospital and Hospital Trauma CoordinationDocument4 paginiPrehospital and Hospital Trauma CoordinationnurulÎncă nu există evaluări
- Nursing Test 4 (NP Iv)Document9 paginiNursing Test 4 (NP Iv)Yuxin LiuÎncă nu există evaluări
- P.E. 2 First Aid Hand OutDocument11 paginiP.E. 2 First Aid Hand OutLaleth Mendoza Ojales100% (3)
- Hernani, Eastern Samar Citizen's Health Charter: Mission: To Sustain An Improved Quality of Life ThroughDocument10 paginiHernani, Eastern Samar Citizen's Health Charter: Mission: To Sustain An Improved Quality of Life ThroughCoreene CularÎncă nu există evaluări
- Initial Assessment and Management: Presented by Fayez Abillama, MDDocument53 paginiInitial Assessment and Management: Presented by Fayez Abillama, MDDaniel GhosseinÎncă nu există evaluări
- Preboard Exam Np3 Medical Surgical NursingDocument19 paginiPreboard Exam Np3 Medical Surgical NursingBhie Bhie100% (1)
- Carnival Medical Positions DetailsDocument6 paginiCarnival Medical Positions DetailsEliseo CastroÎncă nu există evaluări
- 206.05 Aircraft Rescue Fire Fighting ResponsesDocument12 pagini206.05 Aircraft Rescue Fire Fighting ResponsesijejwoirdwqowÎncă nu există evaluări
- The Role, Preparedness and Management of Nurses During Disasters 1325648617Document26 paginiThe Role, Preparedness and Management of Nurses During Disasters 1325648617Pepper Mint0% (1)
- Traditional Ecological Knowledge and Natural Resource ManagementDocument281 paginiTraditional Ecological Knowledge and Natural Resource ManagementShannon FergusonÎncă nu există evaluări
- Reading - Nathavitharana EBioMed 2022Document15 paginiReading - Nathavitharana EBioMed 2022carolÎncă nu există evaluări
- Orientation Booklet For Emergency DepartmentDocument10 paginiOrientation Booklet For Emergency Departmentshahidchaudhary100% (1)
- 9137 Airport Services Manual Part 7 - Airport Emergency PlanningDocument97 pagini9137 Airport Services Manual Part 7 - Airport Emergency PlanningLuiis Cardona100% (6)
- Guidelines For Triage of Obstetric PatientsDocument16 paginiGuidelines For Triage of Obstetric Patientsastroirma0% (2)
- Epidemiology of Traumatic Spinal Cord Injury: A SAARC PerspectiveDocument14 paginiEpidemiology of Traumatic Spinal Cord Injury: A SAARC PerspectivejazelÎncă nu există evaluări
- COVID 19 Pandemic PlanDocument32 paginiCOVID 19 Pandemic PlanElspeth Kernebone83% (12)
- TriageDocument17 paginiTriageAnsari ShariqÎncă nu există evaluări
- Prelims DisasterDocument10 paginiPrelims DisasterBlack TeamÎncă nu există evaluări
- Citizen's CharterDocument12 paginiCitizen's CharterShayne Cabotaje Delos Santos - BorlingÎncă nu există evaluări
- Emergency and Disaster NursingDocument9 paginiEmergency and Disaster NursingDempsey AlmirañezÎncă nu există evaluări
- Merritt-Student ResumeDocument2 paginiMerritt-Student Resumeapi-487044349Încă nu există evaluări
- Support Services SOPDocument18 paginiSupport Services SOPdamarwuÎncă nu există evaluări
- JCI Training Booklet 2020 C PDFDocument94 paginiJCI Training Booklet 2020 C PDFJoan Verano100% (2)