S-ar putea să vă placă și
- Investigation of Fatal Accident on Offshore Oil RigDocument37 paginiInvestigation of Fatal Accident on Offshore Oil RigkfranovskyÎncă nu există evaluări
- Blowout Investigation Brazos Block 417 July 13, 2001Document43 paginiBlowout Investigation Brazos Block 417 July 13, 2001Dan MarrÎncă nu există evaluări
- United States Court of Appeals, Fifth CircuitDocument20 paginiUnited States Court of Appeals, Fifth CircuitScribd Government DocsÎncă nu există evaluări
- Taum Sauk ReportDocument134 paginiTaum Sauk ReportSATEESH KUMAR PURIÎncă nu există evaluări
- SETWAC Minutes 4-25-13Document5 paginiSETWAC Minutes 4-25-13unspamableÎncă nu există evaluări
- Trex 06166Document82 paginiTrex 06166OSDocs2012Încă nu există evaluări
- United States Department The Interior: Office of Inspector General Washington, DC 20240Document12 paginiUnited States Department The Interior: Office of Inspector General Washington, DC 20240marcus1265Încă nu există evaluări
- M/V New Smyrna Inlet (Sample Ultrasonic Hull Survey)Document15 paginiM/V New Smyrna Inlet (Sample Ultrasonic Hull Survey)Suenos AzulesÎncă nu există evaluări
- TRCA DocsDocument24 paginiTRCA DocsGlobal_bureauÎncă nu există evaluări
- Governance Committee For The MPWSP FINAL Agenda Packet 06-24-15Document84 paginiGovernance Committee For The MPWSP FINAL Agenda Packet 06-24-15L. A. PatersonÎncă nu există evaluări
- 4 29 09Document105 pagini4 29 09James DrewÎncă nu există evaluări
- Deepwater AssignmentDocument14 paginiDeepwater Assignmentsam lissen100% (1)
- Red Hill Aoc Section 2 2 Tirm Report 2016-10-11Document246 paginiRed Hill Aoc Section 2 2 Tirm Report 2016-10-11JackÎncă nu există evaluări
- Technical ReportDocument38 paginiTechnical ReportRyan ColemanÎncă nu există evaluări
- Sunseeker Predator SampleDocument98 paginiSunseeker Predator SampleChet Stephens100% (1)
- Investigation of Drill ShipDocument37 paginiInvestigation of Drill Shiptafani electricalÎncă nu există evaluări
- 10000017144Document196 pagini10000017144Chapter 11 DocketsÎncă nu există evaluări
- Luicho News Releasse Final Luicho Drill Result.25.10.2000Document2 paginiLuicho News Releasse Final Luicho Drill Result.25.10.2000Héctor CarrizalesÎncă nu există evaluări
- Action Items 11 - Equipment PreservationDocument6 paginiAction Items 11 - Equipment PreservationMathias OnosemuodeÎncă nu există evaluări
- Plains 2009-0043Document7 paginiPlains 2009-0043algoreÎncă nu există evaluări
- Improving and Streamlining The Coast Guard'S Acquisition ProgramDocument60 paginiImproving and Streamlining The Coast Guard'S Acquisition ProgramScribd Government DocsÎncă nu există evaluări
- Deepwater Horizon investigations uncover multiple causes of Gulf oil spillDocument3 paginiDeepwater Horizon investigations uncover multiple causes of Gulf oil spillAnanth ManoharÎncă nu există evaluări
- 2007 Clear Creek County MinutesDocument825 pagini2007 Clear Creek County MinutesheatherÎncă nu există evaluări
- Cargo Survey SampleDocument8 paginiCargo Survey SampleChet Stephens100% (6)
- MANAGING ABANDONED MINE RISKDocument206 paginiMANAGING ABANDONED MINE RISKPaulo de Tárcio Jr.Încă nu există evaluări
- Deep Water Horizon Oil Spill Incident Franklin County Incident Action PlanDocument5 paginiDeep Water Horizon Oil Spill Incident Franklin County Incident Action PlanMichael AllenÎncă nu există evaluări
- In Re: Governor'S Island Preservation and Education CorporationDocument20 paginiIn Re: Governor'S Island Preservation and Education CorporationCasey SeilerÎncă nu există evaluări
- 10000028244Document213 pagini10000028244Chapter 11 DocketsÎncă nu există evaluări
- Governance Committee Agenda Packet 07-16-14Document239 paginiGovernance Committee Agenda Packet 07-16-14L. A. PatersonÎncă nu există evaluări
- CVO Poly BD Contractor FatalityDocument11 paginiCVO Poly BD Contractor FatalityVasant Kumar VarmaÎncă nu există evaluări
- Establish Recommended American Shipbuilding Quality Standards - Final Report - 1999Document17 paginiEstablish Recommended American Shipbuilding Quality Standards - Final Report - 1999youngfpÎncă nu există evaluări
- Minutes August 21, 2012Document2 paginiMinutes August 21, 2012NorthpithÎncă nu există evaluări
- IAP - 47 20june10Document6 paginiIAP - 47 20june10Michael AllenÎncă nu există evaluări
- Gregg Perkin QualificationsDocument10 paginiGregg Perkin QualificationsOSDocs2012Încă nu există evaluări
- Tim Doodys Southeast Louisiana Flood Protection Authority-Easts InfractionsDocument5 paginiTim Doodys Southeast Louisiana Flood Protection Authority-Easts InfractionsRoyArrigoÎncă nu există evaluări
- Otc 16820 PDFDocument11 paginiOtc 16820 PDFSampurnanand PandeyÎncă nu există evaluări
- Tac Mprwa Minutes 04-04-16Document5 paginiTac Mprwa Minutes 04-04-16L. A. PatersonÎncă nu există evaluări
- Flash Report 15 21june101Document1 paginăFlash Report 15 21june101Michael AllenÎncă nu există evaluări
- fpso-USCG RequirementsDocument17 paginifpso-USCG RequirementsAji VasudevanÎncă nu există evaluări
- Uco Operations 2023, Weekly Lcam Report by Donald Foster, August 6, 2023Document24 paginiUco Operations 2023, Weekly Lcam Report by Donald Foster, August 6, 2023Christine PerryÎncă nu există evaluări
- Safety Culture Lessons from Major AccidentsDocument8 paginiSafety Culture Lessons from Major AccidentsHesham HamyÎncă nu există evaluări
- LNG Offshore Receiving TerminalsDocument54 paginiLNG Offshore Receiving Terminalsdigeca100% (1)
- Iraq Oil TerminalDocument77 paginiIraq Oil Terminalvuong100% (1)
- Deepwater Horizon Accident Investigation Report Executive SummaryDocument6 paginiDeepwater Horizon Accident Investigation Report Executive SummaryJamie TaylorÎncă nu există evaluări
- Trex 50003Document188 paginiTrex 50003OSDocs2012Încă nu există evaluări
- Radiation Technologies Superfund PlanDocument11 paginiRadiation Technologies Superfund PlanLouis C. HochmanÎncă nu există evaluări
- Camp Pendleton ToxicityDocument37 paginiCamp Pendleton ToxicityDavid Lincoln100% (1)
- LNG Offshore Receiving TerminalsDocument54 paginiLNG Offshore Receiving TerminalspoetoetÎncă nu există evaluări
- Gulf of Mexico Restoration: BP Sustainability Reporting 2010Document45 paginiGulf of Mexico Restoration: BP Sustainability Reporting 2010Dragosh Iulian DragosÎncă nu există evaluări
- Capd 000000021Document19 paginiCapd 000000021Capitol Breach DiscoveryÎncă nu există evaluări
- Governance Committee Agenda Packet 08-25-14Document179 paginiGovernance Committee Agenda Packet 08-25-14L. A. PatersonÎncă nu există evaluări
- Arctic Well Integrity and Spill Prevention Methods and TechnologyDocument54 paginiArctic Well Integrity and Spill Prevention Methods and TechnologyMahmoud Abdallah MohamedÎncă nu există evaluări
- Investigation of 2000 Offshore Oil Rig BlowoutDocument16 paginiInvestigation of 2000 Offshore Oil Rig BlowoutasdasdÎncă nu există evaluări
- Responsive Document - CREW: NOAA: Regarding BP Oil Spill: 4/3/2012 - (Part 2) Pages From FOIA 2010-377 ORR OHC Interim 4 1 To 3596 FinalDocument1.000 paginiResponsive Document - CREW: NOAA: Regarding BP Oil Spill: 4/3/2012 - (Part 2) Pages From FOIA 2010-377 ORR OHC Interim 4 1 To 3596 FinalCREWÎncă nu există evaluări
- House Hearing, 109TH Congress - A Review of Ongoing Management Concerns at Los Alamos National LaboratoryDocument53 paginiHouse Hearing, 109TH Congress - A Review of Ongoing Management Concerns at Los Alamos National LaboratoryScribd Government DocsÎncă nu există evaluări
- Why Only Two FPSOs in U.S. Gulf of Mexico?: The Late Start and Twenty Year SagaDe la EverandWhy Only Two FPSOs in U.S. Gulf of Mexico?: The Late Start and Twenty Year SagaÎncă nu există evaluări
- Navigation Rules and Regulations Handbook: International—InlandDe la EverandNavigation Rules and Regulations Handbook: International—InlandEvaluare: 5 din 5 stele5/5 (1)
- The Fossil Fuel Revolution: Shale Gas and Tight OilDe la EverandThe Fossil Fuel Revolution: Shale Gas and Tight OilÎncă nu există evaluări
- Nuggets to Neutrinos: The Homestake StoryDe la EverandNuggets to Neutrinos: The Homestake StoryEvaluare: 5 din 5 stele5/5 (2)
- U.S. Army Guide to Military MountaineeringDe la EverandU.S. Army Guide to Military MountaineeringÎncă nu există evaluări
- Safety Alert: Stabbing Board Related IncidentsDocument1 paginăSafety Alert: Stabbing Board Related IncidentsHany AhmedÎncă nu există evaluări
- S WeatherfDocument3 paginiS WeatherfHany AhmedÎncă nu există evaluări
- Critical AreaDocument2 paginiCritical AreaHany AhmedÎncă nu există evaluări
- Fishbone RevisedDocument3 paginiFishbone RevisedHany AhmedÎncă nu există evaluări
- Jereh ElevatorDocument4 paginiJereh ElevatorHany AhmedÎncă nu există evaluări
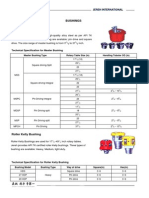
- Bushings Master BushingDocument2 paginiBushings Master BushingHany AhmedÎncă nu există evaluări
- Oilfield JetlubeDocument24 paginiOilfield JetlubeHany AhmedÎncă nu există evaluări
- Critical Area Drawings: Document Number 50000805-MAN-001 Revision A 64 of 66Document2 paginiCritical Area Drawings: Document Number 50000805-MAN-001 Revision A 64 of 66Hany AhmedÎncă nu există evaluări
- Guidance For RcaDocument12 paginiGuidance For RcaHany AhmedÎncă nu există evaluări
- GrantPrideco Drill Pipe Data TablesDocument24 paginiGrantPrideco Drill Pipe Data TablesMaximo Biarrieta RodriguezÎncă nu există evaluări
- Stabbing BoardsDocument2 paginiStabbing BoardsHany AhmedÎncă nu există evaluări
- Jet Lube Jet Lok IIDocument2 paginiJet Lube Jet Lok IIHany Ahmed0% (1)
- API Tubing Table SpecificationsDocument6 paginiAPI Tubing Table SpecificationsDavid KusumaÎncă nu există evaluări
- Радиус-Сервис - Products - JarsDocument4 paginiРадиус-Сервис - Products - JarsHany AhmedÎncă nu există evaluări
- Радиус-Сервис - Products - Shock ToolsDocument2 paginiРадиус-Сервис - Products - Shock ToolsHany AhmedÎncă nu există evaluări
- 758 42000e Testork Revd LoresDocument4 pagini758 42000e Testork Revd LoresHany AhmedÎncă nu există evaluări
- Hydraulic - Mechanical Drilling Jar (HMJ) - Downhole Drilling ToolsDocument4 paginiHydraulic - Mechanical Drilling Jar (HMJ) - Downhole Drilling ToolsHany AhmedÎncă nu există evaluări
- Spider Varco 375Document1 paginăSpider Varco 375Hany AhmedÎncă nu există evaluări
- Shock Tool - Downhole Drilling ToolsDocument4 paginiShock Tool - Downhole Drilling ToolsHany AhmedÎncă nu există evaluări
- Challenger Bumper Jar - Downhole Drilling ToolsDocument3 paginiChallenger Bumper Jar - Downhole Drilling ToolsHany AhmedÎncă nu există evaluări
- High Output Hydraulic - Mechanical Drilling Jar - (HO-HMJ) - Downhole Drilling ToolsDocument4 paginiHigh Output Hydraulic - Mechanical Drilling Jar - (HO-HMJ) - Downhole Drilling ToolsHany AhmedÎncă nu există evaluări
- Hydraulic - Mechanical Drilling Jar (HMJ) - Downhole Drilling ToolsDocument4 paginiHydraulic - Mechanical Drilling Jar (HMJ) - Downhole Drilling ToolsHany AhmedÎncă nu există evaluări
- Tianhe Oil Group Huifeng Petroleum Equipment Co - pdf2Document3 paginiTianhe Oil Group Huifeng Petroleum Equipment Co - pdf2Hany AhmedÎncă nu există evaluări
- Tianhe Oil Group Huifeng Petroleum Equipment Co - pdf1Document3 paginiTianhe Oil Group Huifeng Petroleum Equipment Co - pdf1Hany AhmedÎncă nu există evaluări
- Jar Pro Drillstring Jarring Analysis SoftwareDocument5 paginiJar Pro Drillstring Jarring Analysis SoftwareHany AhmedÎncă nu există evaluări
- Tianhe Oil Group Huifeng Petroleum Equipment CoDocument3 paginiTianhe Oil Group Huifeng Petroleum Equipment CoHany AhmedÎncă nu există evaluări
- Tianhe Oil Group Huifeng Petroleum Equipment Co - pdf4Document3 paginiTianhe Oil Group Huifeng Petroleum Equipment Co - pdf4Hany AhmedÎncă nu există evaluări
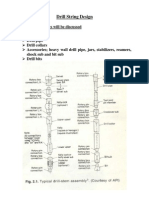
- Drill String DesignDocument12 paginiDrill String DesignAsaadgz100% (1)
- Pumps Motors AssDocument57 paginiPumps Motors AssHany AhmedÎncă nu există evaluări
- ESC&AWK Operation&Maintenance ManualDocument21 paginiESC&AWK Operation&Maintenance ManualWander GomesÎncă nu există evaluări
- Electromechanical Conveyance Systems: Unit-IVDocument74 paginiElectromechanical Conveyance Systems: Unit-IVsofiyaÎncă nu există evaluări
- Topic 7 - Mechanical Transportation SystemDocument62 paginiTopic 7 - Mechanical Transportation SystemELVEVIYONA JOOTÎncă nu există evaluări
- Selection Guide Fluid Coupling NewDocument34 paginiSelection Guide Fluid Coupling NewIsaac Montero Barrera100% (1)
- August 1, 2015Document14 paginiAugust 1, 2015The Delphos HeraldÎncă nu există evaluări
- Unit 1 Teamwork: Jobs and ExperienceDocument21 paginiUnit 1 Teamwork: Jobs and ExperienceQuan NguyenÎncă nu există evaluări
- Ops 0055 July 12016Document164 paginiOps 0055 July 12016Aizat NajibÎncă nu există evaluări
- Eriez Sl08 Lifting Magnets BrochureDocument24 paginiEriez Sl08 Lifting Magnets Brochuredante224Încă nu există evaluări
- USAS 856.1-1969 Safety Standard for Powered Industrial TrucksDocument65 paginiUSAS 856.1-1969 Safety Standard for Powered Industrial TrucksRethfo A Riquelme CastilloÎncă nu există evaluări
- Mpu2in 02Document51 paginiMpu2in 02vbamain50% (2)
- Vertical Transportation SystemDocument14 paginiVertical Transportation Systempassionpropel100% (3)
- Dannmar: Sx-6/Xl User ManualDocument36 paginiDannmar: Sx-6/Xl User Manuallalit PatilÎncă nu există evaluări
- Installation, Operation, and Maintenance Manual: Model 3409Document72 paginiInstallation, Operation, and Maintenance Manual: Model 3409MaintenanceÎncă nu există evaluări
- Installation and Operation ManualDocument56 paginiInstallation and Operation Manualfarichtape channelÎncă nu există evaluări
- Brochure Drilling WebDocument17 paginiBrochure Drilling WebDan BanulÎncă nu există evaluări
- Machine-Room-Less Elevator: in Compliance With The Standards of EN81-20 and EN81-50Document27 paginiMachine-Room-Less Elevator: in Compliance With The Standards of EN81-20 and EN81-50Martin PortilloÎncă nu există evaluări
- Ceng 7509. Bridge Engineering: Dr. John, Me, Mba, PHD, Ce, Mie, FivDocument80 paginiCeng 7509. Bridge Engineering: Dr. John, Me, Mba, PHD, Ce, Mie, FivTesfamichael Abathun100% (1)
- Boiler Ash Handling Operation & Maintenance PDFDocument64 paginiBoiler Ash Handling Operation & Maintenance PDFdreamboy87Încă nu există evaluări
- Housing Case StudyDocument40 paginiHousing Case StudyRishu Dev100% (1)
- LIFTS: A HISTORY AND GUIDE TO BUILDING TRANSPORTATION SYSTEMSDocument44 paginiLIFTS: A HISTORY AND GUIDE TO BUILDING TRANSPORTATION SYSTEMSmahboob2Încă nu există evaluări
- Torin 2-Ton Hydraulic Trolley Jack ManualDocument6 paginiTorin 2-Ton Hydraulic Trolley Jack ManualWIRAKOCHAÎncă nu există evaluări
- 16 Screw Hoist For Sluice Gate PDFDocument10 pagini16 Screw Hoist For Sluice Gate PDFsamÎncă nu există evaluări
- M984A1Document713 paginiM984A1Joffre Lautaro Benavides SeminarioÎncă nu există evaluări
- Fire Safety Design GuideDocument19 paginiFire Safety Design GuideZulvita AmandaÎncă nu există evaluări
- Vertical Transportation Solutions Manual V0Document125 paginiVertical Transportation Solutions Manual V0ERCAN ÖZERDEN100% (1)
- Ansi A10 5 2006Document32 paginiAnsi A10 5 2006Faouzi SouissiÎncă nu există evaluări
- PLC Traction User Manual PDFDocument131 paginiPLC Traction User Manual PDFfreddyjoertyÎncă nu există evaluări
- FOKKER 28 MK 100 Crew Coordination DocumentDocument60 paginiFOKKER 28 MK 100 Crew Coordination Documentvictor50550% (2)
- ITP Crane - Pertamina EPDocument14 paginiITP Crane - Pertamina EPAry Putra100% (4)
- TroubleshootingDocument24 paginiTroubleshootingAamer Khawaja100% (1)