S-ar putea să vă placă și
- ICU Drips: Stephanie Sanderson, RN, MSN, CNS, CCNS, CCRN Medical Cardiac ICU-UNMHDocument32 paginiICU Drips: Stephanie Sanderson, RN, MSN, CNS, CCNS, CCRN Medical Cardiac ICU-UNMHNicole Adkins100% (1)
- ACLS DrugDocument7 paginiACLS DrugPhongsatorn Thunin100% (1)
- ACLS Advanced Cardiovascular Life Support Provider Manual 2023De la EverandACLS Advanced Cardiovascular Life Support Provider Manual 2023Încă nu există evaluări
- Alert Medical Series: Emergency Medicine Alert IIIDe la EverandAlert Medical Series: Emergency Medicine Alert IIIÎncă nu există evaluări
- ACLS PharmacologyDocument5 paginiACLS PharmacologyKuruva MallikarjunaÎncă nu există evaluări
- ACLS Full Lesson Plans PDFDocument60 paginiACLS Full Lesson Plans PDFVictoriano Mendez100% (1)
- ACLS MneumonicsDocument4 paginiACLS MneumonicsnaranothÎncă nu există evaluări
- ACLS Study Guide: Ecg Strip InterpretationDocument12 paginiACLS Study Guide: Ecg Strip InterpretationMariana Berger100% (1)
- 2016 Updated ACLS HandoutsDocument24 pagini2016 Updated ACLS Handoutskarenjlazarus86% (14)
- Study Guide: MandatoryDocument24 paginiStudy Guide: Mandatorybooksir86% (7)
- ACLS Simulation ScenariosDocument14 paginiACLS Simulation ScenariosVanessa HermioneÎncă nu există evaluări
- ACLS PharmacologyDocument6 paginiACLS PharmacologyEunice Angela Fulgueras80% (5)
- PALS Interim Material 2020 - Provider Manual ChangesDocument3 paginiPALS Interim Material 2020 - Provider Manual ChangesyossyusÎncă nu există evaluări
- Paramedic Pediatric Scenario 2017Document3 paginiParamedic Pediatric Scenario 2017Chad StreetÎncă nu există evaluări
- Acls MegacodeDocument8 paginiAcls Megacodes33d_destinyÎncă nu există evaluări
- Introd To ECG Code Blue Champs March 2019Document52 paginiIntrod To ECG Code Blue Champs March 2019james rukenya100% (1)
- ACLS (Advanced Cardiac Life Support) Algorithms & NotesDocument4 paginiACLS (Advanced Cardiac Life Support) Algorithms & Notesiamlucil100% (4)
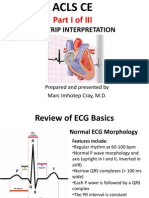
- ACLS CE-Part I of III - ECG Strip Interpretation W Case Scenarios SupplementalDocument80 paginiACLS CE-Part I of III - ECG Strip Interpretation W Case Scenarios SupplementalMarc Imhotep Cray, M.D.100% (2)
- 15 Item ACLS Drill With RationaleDocument12 pagini15 Item ACLS Drill With RationaleLj Ferolino100% (1)
- ACLS Pretest Exam AnnotatedDocument21 paginiACLS Pretest Exam AnnotatedMOLLYÎncă nu există evaluări
- AclsDocument62 paginiAclsAlemayehu beharuÎncă nu există evaluări
- ACLS DrugsDocument16 paginiACLS Drugstostc100% (2)
- ACLS Study Guide NewDocument35 paginiACLS Study Guide NewNIRANJANA SHALINIÎncă nu există evaluări
- Drug Card Emergency DepartmentDocument2 paginiDrug Card Emergency Departmentdrmohdtanveer100% (3)
- ACLS Study Guide JULY 2021 UPDATEDocument3 paginiACLS Study Guide JULY 2021 UPDATENina Morada100% (2)
- AclsDocument73 paginiAclsKamel Hady50% (2)
- FREE 2022 ACLS Study Guide - ACLS Made Easy! PDFDocument18 paginiFREE 2022 ACLS Study Guide - ACLS Made Easy! PDFkumar23Încă nu există evaluări
- Acls Pretest Answer Key: Rhythm Identification (Part I)Document3 paginiAcls Pretest Answer Key: Rhythm Identification (Part I)aditÎncă nu există evaluări
- ACLS Study GuideDocument28 paginiACLS Study GuideNicole Berry100% (1)
- Pharmacological Tools: Doses, Routes, and Uses of Common DrugDocument1 paginăPharmacological Tools: Doses, Routes, and Uses of Common DrugApuntesdemedicinaa blogÎncă nu există evaluări
- The Crash CartDocument39 paginiThe Crash Cartpramod kumawat100% (1)
- PALS Study Guide: 2020 GuidelinesDocument3 paginiPALS Study Guide: 2020 GuidelinesVictoria Kidd100% (2)
- Cals ReviewbjvjvjDocument14 paginiCals ReviewbjvjvjCarl Jay M Ocariza100% (1)
- Acls DrugsDocument5 paginiAcls DrugsDebby Christiana SÎncă nu există evaluări
- ACLS and MegacodeDocument33 paginiACLS and MegacodeMark Joseph100% (1)
- 15 Item Acls DrillDocument4 pagini15 Item Acls DrillVal SolidumÎncă nu există evaluări
- PALS Pre StudyDocument28 paginiPALS Pre Studynursesed100% (7)
- ACLSDocument17 paginiACLSms_lezah100% (4)
- ACLS Algorithms SlideDocument26 paginiACLS Algorithms SlidehrsoÎncă nu există evaluări
- Pediatric Advanced Life Support: I. PALS System Approach AlgorithmDocument19 paginiPediatric Advanced Life Support: I. PALS System Approach AlgorithmIsabel Castillo100% (1)
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesDe la EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesEvaluare: 4 din 5 stele4/5 (6)
- ACLS Algorithms 2020 (Advanced Cardiac Life Support)Document1 paginăACLS Algorithms 2020 (Advanced Cardiac Life Support)evelyn k100% (2)
- ACLSDocument46 paginiACLSYeoh Hong Shin100% (3)
- Aha Acls Prep Packet 2021 NewDocument69 paginiAha Acls Prep Packet 2021 Newdim100% (2)
- ACLS Provider Manual Supplementary Material: © 2020 American Heart AssociationDocument75 paginiACLS Provider Manual Supplementary Material: © 2020 American Heart AssociationpolelÎncă nu există evaluări
- ACLS Practical Case Scenarios (1 June 2011)Document15 paginiACLS Practical Case Scenarios (1 June 2011)nersÎncă nu există evaluări
- Acls LectureDocument15 paginiAcls LectureVincent BautistaÎncă nu există evaluări
- ACLS Precourse Test AnswersDocument60 paginiACLS Precourse Test AnswersTip Piraya60% (5)
- CPR ACLS Study GuideDocument18 paginiCPR ACLS Study GuideJohn Phamacy100% (1)
- AclsDocument11 paginiAclsdyah rahayu hutamiÎncă nu există evaluări
- Emergency Department Resuscitation of the Critically Ill, 2nd Edition: A Crash Course in Critical CareDe la EverandEmergency Department Resuscitation of the Critically Ill, 2nd Edition: A Crash Course in Critical CareÎncă nu există evaluări
- Advance Cardiac Life Support: Short, Sweet and to the PointDe la EverandAdvance Cardiac Life Support: Short, Sweet and to the PointEvaluare: 3 din 5 stele3/5 (2)
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!De la EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Încă nu există evaluări
- Pediatric Advanced Life Support (PALS) Provider HandbookDe la EverandPediatric Advanced Life Support (PALS) Provider HandbookÎncă nu există evaluări
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDe la EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsÎncă nu există evaluări
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesDe la EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesEvaluare: 5 din 5 stele5/5 (2)
- The Establishment of A No Interruption Zone During Medication Preparation Decreases Unnecessary Interruptions Thereby Increasing Patient Safety.Document3 paginiThe Establishment of A No Interruption Zone During Medication Preparation Decreases Unnecessary Interruptions Thereby Increasing Patient Safety.LaineyMarie1Încă nu există evaluări
- Drug Study: Nursing DepartmentDocument1 paginăDrug Study: Nursing Departmentgiselle chloe100% (1)
- Hypertension G P New Dr. Anidu PathiranaDocument79 paginiHypertension G P New Dr. Anidu PathiranaNalin WickramasingheÎncă nu există evaluări
- Navigation Search THC (Disambiguation) : TetrahydrocannabinolDocument14 paginiNavigation Search THC (Disambiguation) : TetrahydrocannabinolVictor Vacariu100% (1)
- C-10 Ointment 2Document90 paginiC-10 Ointment 2Mara Angelica100% (1)
- Otc Advisor PainDocument24 paginiOtc Advisor Painfarzad100% (2)
- Asap PMP V4.1 10.1810Document46 paginiAsap PMP V4.1 10.1810Kon Fung DharmaÎncă nu există evaluări
- Medical Surgical Nursing NotesDocument66 paginiMedical Surgical Nursing Notessimon92% (12)
- Color Code Anesthesia PDFDocument6 paginiColor Code Anesthesia PDFYusnia Gulfa MaharaniÎncă nu există evaluări
- Famotidine (Pepcid)Document1 paginăFamotidine (Pepcid)E100% (1)
- Floating Effervescent Tablets A ReviewDocument6 paginiFloating Effervescent Tablets A ReviewsherepunjabÎncă nu există evaluări
- Chapter 1 Hospital PharmacyDocument3 paginiChapter 1 Hospital PharmacyPatrisha Bello BulacanÎncă nu există evaluări
- Ibuprofen Farmakologi 3Document7 paginiIbuprofen Farmakologi 3Shafira TamaraÎncă nu există evaluări
- Potential of Piperine As A Bioavailability Enhancer: Vasika LeavesDocument10 paginiPotential of Piperine As A Bioavailability Enhancer: Vasika LeavesSushilkumar ShindeÎncă nu există evaluări
- Amfetamine 2Document9 paginiAmfetamine 2Cassandra Moore100% (1)
- Pharm Quiz 1Document59 paginiPharm Quiz 1Anonymous vXOM1Wxt100% (1)
- Formularium Obat RSDocument2 paginiFormularium Obat RSMyzard AriefÎncă nu există evaluări
- SOP Farmasi1Document54 paginiSOP Farmasi1Reny KridayantiÎncă nu există evaluări
- High Alert DrugsDocument17 paginiHigh Alert DrugsAndrean Mukti BeladexsaÎncă nu există evaluări
- Lista TAB 01.02.2018Document40 paginiLista TAB 01.02.2018Botezatu VilusaÎncă nu există evaluări
- Acute Management of Pediatric Cyclic Vomiting Syndrome A Systematic ReviewDocument11 paginiAcute Management of Pediatric Cyclic Vomiting Syndrome A Systematic ReviewNanda WibowoÎncă nu există evaluări
- PNF July2019Document63 paginiPNF July2019ldh pharmacyÎncă nu există evaluări
- Price List Harga Jadi DR - Agus (Wahau)Document12 paginiPrice List Harga Jadi DR - Agus (Wahau)duwiÎncă nu există evaluări
- Designer Drugs: K2/Spice, Bath Salts, Molly and OthersDocument9 paginiDesigner Drugs: K2/Spice, Bath Salts, Molly and OtherstadcpÎncă nu există evaluări
- Psychiatric Treatment of Children and AdolescentsDocument15 paginiPsychiatric Treatment of Children and Adolescentsiyuzaim02Încă nu există evaluări
- 1-An Overview of Community PharmacyDocument55 pagini1-An Overview of Community PharmacyekramÎncă nu există evaluări
- TIKOSYN Treatment GuidelinesDocument8 paginiTIKOSYN Treatment GuidelinesrbmartinivÎncă nu există evaluări
- Tetracycline HCL Drug StudyDocument4 paginiTetracycline HCL Drug StudyCheezy BreadÎncă nu există evaluări
- Which UTI Therapies Are Safe and Effective During Breastfeeding?Document3 paginiWhich UTI Therapies Are Safe and Effective During Breastfeeding?Naila Shofwati PutriÎncă nu există evaluări
- Gastritis 508Document8 paginiGastritis 508FaichalMartadinataÎncă nu există evaluări