S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Medical Anthropology Study of The Ebola Virus Disease (EVD) Outbreak in Liberia/West AfricaDocument21 paginiMedical Anthropology Study of The Ebola Virus Disease (EVD) Outbreak in Liberia/West AfricaJoy AraújoÎncă nu există evaluări
- Curs Engleza 2014 PDFDocument263 paginiCurs Engleza 2014 PDFDeea TrancăÎncă nu există evaluări
- Clinical Epidemioogy Lecture Series 1Document92 paginiClinical Epidemioogy Lecture Series 1Kato CalebÎncă nu există evaluări
- Home Health National Patient Safety GoalsDocument3 paginiHome Health National Patient Safety Goalsjenn1722Încă nu există evaluări
- Typhoid Fever: Pathognomonic SignDocument2 paginiTyphoid Fever: Pathognomonic SignLylibeth Anne CalimlimÎncă nu există evaluări
- Project Report On Menstrual HygeineDocument33 paginiProject Report On Menstrual HygeineavnishÎncă nu există evaluări
- Local Treatment With A Polycarbophil-Based Cream in Postmenopausal Women With Genitourinary Syndrome of MenopauseDocument6 paginiLocal Treatment With A Polycarbophil-Based Cream in Postmenopausal Women With Genitourinary Syndrome of MenopauseBerry BancinÎncă nu există evaluări
- Depot-Medroxyprogesterone Acetate Injection Depo-ProveraDocument13 paginiDepot-Medroxyprogesterone Acetate Injection Depo-Proverarestu pangestutiÎncă nu există evaluări
- Managing Fatigue During PregnancyDocument2 paginiManaging Fatigue During PregnancyBlanz Irybelle KindomÎncă nu există evaluări
- Veneracion NCP 1Document2 paginiVeneracion NCP 1Romm JacobÎncă nu există evaluări
- Gastroenteritis HistoryDocument8 paginiGastroenteritis HistoryLeefre Mae D NermalÎncă nu există evaluări
- Health: at The Docotr'SDocument2 paginiHealth: at The Docotr'SNatalli MichiganÎncă nu există evaluări
- Clara Louis Maas nurse volunteer who died in yellow fever experimentDocument11 paginiClara Louis Maas nurse volunteer who died in yellow fever experimentClarissa Guifaya50% (2)
- COVID-19 Schools Summary PDFDocument18 paginiCOVID-19 Schools Summary PDFActionNewsJaxÎncă nu există evaluări
- p1725 Chapter 10 SlidesDocument33 paginip1725 Chapter 10 Slideszhaza afilillaÎncă nu există evaluări
- COVID-19 Prevention & IEC Committee, PGIMER Chandigarh: Tentative Webinar Schedule For Healthcare ProfessionalsDocument3 paginiCOVID-19 Prevention & IEC Committee, PGIMER Chandigarh: Tentative Webinar Schedule For Healthcare Professionalsvarshasharma05Încă nu există evaluări
- Teaching Plan About Conjunctivitis: Haemophilus InfluenzaeDocument3 paginiTeaching Plan About Conjunctivitis: Haemophilus InfluenzaeJanaica Juan100% (1)
- Communication Scenarios PDFDocument1.052 paginiCommunication Scenarios PDFDr AhmedÎncă nu există evaluări
- Unit 6 EbolaDocument6 paginiUnit 6 Ebolaapi-275689851Încă nu există evaluări
- Outbreak InvestigationDocument35 paginiOutbreak Investigationkedar karki100% (2)
- Mirena BrochureDocument24 paginiMirena BrochureNamrata HarishÎncă nu există evaluări
- Counselling and Recent Advancements in Contraceptive DevicesDocument45 paginiCounselling and Recent Advancements in Contraceptive DevicesSweety Yadav100% (1)
- Ultrasound Report for 33 Week PregnancyDocument1 paginăUltrasound Report for 33 Week PregnancyAUSTRIAN DIAGNOSTIC CENTERÎncă nu există evaluări
- Infant Feeding in The Context of HIV InfectionDocument37 paginiInfant Feeding in The Context of HIV InfectionDengAwutÎncă nu există evaluări
- Infeksi NosokomialDocument29 paginiInfeksi NosokomialAlunaficha Melody KiraniaÎncă nu există evaluări
- Industrialrevolutionwikiresearch JaydemengDocument6 paginiIndustrialrevolutionwikiresearch Jaydemengapi-311737472Încă nu există evaluări
- Sheehy 2023 Oi 231248 1698936187.02795Document12 paginiSheehy 2023 Oi 231248 1698936187.02795ABC Action NewsÎncă nu există evaluări
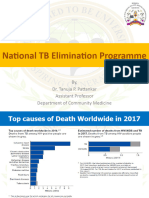
- 28.04.2021 NTEP - RNTCP Dr. Tanuja PattankarDocument29 pagini28.04.2021 NTEP - RNTCP Dr. Tanuja PattankarTanuja PattankarÎncă nu există evaluări
- 099 - VaccinesDocument4 pagini099 - VaccinesArjan LallÎncă nu există evaluări
- Prova Formosa 2019-2Document26 paginiProva Formosa 2019-2Victor FariasÎncă nu există evaluări