S-ar putea să vă placă și
- Direct Posterior Composite 1Document33 paginiDirect Posterior Composite 1Rawzh Salih MuhammadÎncă nu există evaluări
- Aesthetic Layering TechniqueDocument0 paginiAesthetic Layering Techniqueatul_singh2001Încă nu există evaluări
- Avoiding and Treating Dental Complications: Best Practices in DentistryDe la EverandAvoiding and Treating Dental Complications: Best Practices in DentistryDeborah A. TermeieÎncă nu există evaluări
- Fixed Orthodontic Appliances: A Practical GuideDe la EverandFixed Orthodontic Appliances: A Practical GuideEvaluare: 1 din 5 stele1/5 (1)
- Application of the Neutral Zone in ProsthodonticsDe la EverandApplication of the Neutral Zone in ProsthodonticsÎncă nu există evaluări
- Fundamentals of Tooth PreparationDocument50 paginiFundamentals of Tooth Preparationمعاذ نوري محمدÎncă nu există evaluări
- 7 - DrAbeer's Lecture (Dental Cements & Cementation Procedures) PDFDocument51 pagini7 - DrAbeer's Lecture (Dental Cements & Cementation Procedures) PDFTasneem ShamaliÎncă nu există evaluări
- (RestoDent) Components of Cavity PrepDocument47 pagini(RestoDent) Components of Cavity PrepZara Sebastianne GarciaÎncă nu există evaluări
- Managing Dental EmergenciesDocument46 paginiManaging Dental EmergenciesBoris AbayevÎncă nu există evaluări
- Cavity Preparation For Composite RestorationDocument47 paginiCavity Preparation For Composite RestorationDeepak Raisingani100% (1)
- DFG - Total ClassDocument37 paginiDFG - Total ClassSiva RamÎncă nu există evaluări
- Class I and II Indirect Tooth-Colored Restorations (4,5)Document133 paginiClass I and II Indirect Tooth-Colored Restorations (4,5)Samah SakerÎncă nu există evaluări
- Dental Restoration or Dental Filling: Elaborate: Ceban Gabriela Teacher: Doronin NataliaDocument12 paginiDental Restoration or Dental Filling: Elaborate: Ceban Gabriela Teacher: Doronin NataliaGabriela CebanÎncă nu există evaluări
- Non Surgical Endodontic Retreatment: Presented byDocument58 paginiNon Surgical Endodontic Retreatment: Presented bySayak GuptaÎncă nu există evaluări
- Glass Ionomer Powerpoint PresentationDocument59 paginiGlass Ionomer Powerpoint Presentationduracell19100% (1)
- S - 10 Direct Filling GoldDocument30 paginiS - 10 Direct Filling GoldShaliniÎncă nu există evaluări
- Abrasive Agents in DentistryDocument38 paginiAbrasive Agents in Dentistryjohn mwambu100% (1)
- Access CavityDocument35 paginiAccess CavitySaca AnastasiaÎncă nu există evaluări
- Smear LayerDocument114 paginiSmear LayerAME DENTAL COLLEGE RAICHUR, KARNATAKAÎncă nu există evaluări
- Cavity PreparationDocument57 paginiCavity PreparationPrakuz Harmony SubedifiedÎncă nu există evaluări
- Kutler's Thery PDFDocument10 paginiKutler's Thery PDFSam RoyÎncă nu există evaluări
- External Cervical Resorption JC FinalDocument46 paginiExternal Cervical Resorption JC FinalKomal JadhavÎncă nu există evaluări
- 15.1 Root Canal SealersDocument48 pagini15.1 Root Canal SealersRevathy M NairÎncă nu există evaluări
- New Advances in Caries RemovalDocument45 paginiNew Advances in Caries Removalyogi_2311Încă nu există evaluări
- EnamelDocument9 paginiEnamelhustla7100% (1)
- Monoblocks in Root CanalsDocument57 paginiMonoblocks in Root CanalsManva Monish100% (1)
- Inlays and Onlays ReportDocument32 paginiInlays and Onlays ReportAlnielJoManlapigÎncă nu există evaluări
- Lecture 5 Laser in Operative DentistryDocument7 paginiLecture 5 Laser in Operative DentistryDt omarÎncă nu există evaluări
- 17 Fracture MechanicsDocument16 pagini17 Fracture MechanicsRevathy M NairÎncă nu există evaluări
- Anatomy of Apical-Third of Root CanalDocument5 paginiAnatomy of Apical-Third of Root Canalphilo talkÎncă nu există evaluări
- Caries Diagnosis & Caries Risk Assessment: Dr.G.Thiruvenkadam Post Graduate Department of Pediatric DentistryDocument104 paginiCaries Diagnosis & Caries Risk Assessment: Dr.G.Thiruvenkadam Post Graduate Department of Pediatric Dentistryதிருவேங்கடம் கோபாலன்Încă nu există evaluări
- Soumya S Jeena Profile BookDocument53 paginiSoumya S Jeena Profile BooksoumyaÎncă nu există evaluări
- Speeds in DentistryDocument38 paginiSpeeds in DentistryRiya Jain100% (1)
- 12 Pin Retained RestorationDocument59 pagini12 Pin Retained RestorationMohsin HabibÎncă nu există evaluări
- Rootcanalpreparationtechniques 140829191526 Phpapp01Document40 paginiRootcanalpreparationtechniques 140829191526 Phpapp01DrSukesh Upare Phd100% (2)
- Crowns in Pediatric DentistryDocument118 paginiCrowns in Pediatric DentistryAME DENTAL COLLEGE RAICHUR, KARNATAKAÎncă nu există evaluări
- Perforations & ManagementDocument163 paginiPerforations & ManagementAPARNA AARATHI SREEKUMARÎncă nu există evaluări
- CADCAM Vs Traditional Ceramic InlayDocument10 paginiCADCAM Vs Traditional Ceramic InlayAya Ibrahim YassinÎncă nu există evaluări
- Etched Cast RestorationsDocument74 paginiEtched Cast RestorationsMNSÎncă nu există evaluări
- Amalgam BondingDocument21 paginiAmalgam BondingSaad Tanvir ShaikhÎncă nu există evaluări
- C-Shaped Canal ClassificationDocument7 paginiC-Shaped Canal ClassificationPrabu MuthusamyÎncă nu există evaluări
- Wax PatternDocument34 paginiWax PatternMariam SherifÎncă nu există evaluări
- Traumatic Injuries Notes 22nk8pfDocument16 paginiTraumatic Injuries Notes 22nk8pfAmee PatelÎncă nu există evaluări
- The Optical Characteristics of Natural TeethDocument5 paginiThe Optical Characteristics of Natural TeethMarina CretuÎncă nu există evaluări
- Recent Advances in CompositesDocument6 paginiRecent Advances in Compositesanshumankhaitan100% (1)
- Hybrid Ceramics in Dentistry: A Literature ReviewDocument5 paginiHybrid Ceramics in Dentistry: A Literature ReviewNguyên TrầnÎncă nu există evaluări
- Endo Pre FinalsDocument18 paginiEndo Pre FinalsRayne Gelle100% (2)
- Post and Core Orthodontic Courses by Indian Dental AcademyDocument46 paginiPost and Core Orthodontic Courses by Indian Dental AcademyPadmini Reddy100% (1)
- Slide - 11 - Procedural AccidentsDocument31 paginiSlide - 11 - Procedural AccidentsCWT2010100% (1)
- All Ceramic Materials and SystemsDocument6 paginiAll Ceramic Materials and SystemsMahaAhmedÎncă nu există evaluări
- Composites 2Document30 paginiComposites 2Monica RoopChanderÎncă nu există evaluări
- Silorane CompztDocument5 paginiSilorane CompztNaila AmanÎncă nu există evaluări
- Quantec™ System: Graduating TapersDocument7 paginiQuantec™ System: Graduating TapersMonica Agustine HartonoÎncă nu există evaluări
- Pin Amalgam RestorationDocument62 paginiPin Amalgam RestorationRaj JoyÎncă nu există evaluări
- Tarnish and Corrosion / Orthodontic Courses by Indian Dental AcademyDocument20 paginiTarnish and Corrosion / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- Cleaning and Shaping of Root Canal SystemDocument81 paginiCleaning and Shaping of Root Canal SystemToni MaddoxÎncă nu există evaluări
- Indirect Composite Inlay and OnlaysDocument6 paginiIndirect Composite Inlay and OnlaysAdrian DjohanÎncă nu există evaluări
- Apex Locators and Tri Auto ZXDocument5 paginiApex Locators and Tri Auto ZXNasrrashad HashemÎncă nu există evaluări
- Criteria of SelectionDocument12 paginiCriteria of SelectionVinisha Vipin SharmaÎncă nu există evaluări
- Diff Betwn Inlay and Amalgam CavityDocument7 paginiDiff Betwn Inlay and Amalgam CavityVinisha Vipin Sharma100% (1)
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDocument6 paginiNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaÎncă nu există evaluări
- Some Basics of LasersDocument102 paginiSome Basics of LasersVinisha Vipin SharmaÎncă nu există evaluări
- Challenges in Working Length DeterminationDocument101 paginiChallenges in Working Length DeterminationVinisha Vipin SharmaÎncă nu există evaluări
- Acupuncture in Dentistry PDFDocument73 paginiAcupuncture in Dentistry PDFVinisha Vipin SharmaÎncă nu există evaluări
- Mechanical Preparation Updated May2017 Prof Marco VersianiDocument159 paginiMechanical Preparation Updated May2017 Prof Marco VersianiVinisha Vipin SharmaÎncă nu există evaluări
- Laser in Conservative Dentistry & EndodonticsDocument75 paginiLaser in Conservative Dentistry & EndodonticsVinisha Vipin SharmaÎncă nu există evaluări
- Eaat 14 I 1 P 217Document6 paginiEaat 14 I 1 P 217Vinisha Vipin SharmaÎncă nu există evaluări
- Content ServerDocument5 paginiContent ServerVinisha Vipin SharmaÎncă nu există evaluări
- Content ServerDocument6 paginiContent ServerVinisha Vipin SharmaÎncă nu există evaluări
- Glide Path PreparationDocument5 paginiGlide Path PreparationVinisha Vipin SharmaÎncă nu există evaluări
- Show TextDocument1 paginăShow TextVinisha Vipin SharmaÎncă nu există evaluări
- EchsDocument20 paginiEchsVinisha Vipin SharmaÎncă nu există evaluări
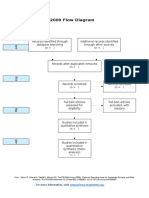
- PRISMA 2009 Flow Diagram: For More Information, VisitDocument1 paginăPRISMA 2009 Flow Diagram: For More Information, VisitVinisha Vipin SharmaÎncă nu există evaluări
- Practice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportDocument5 paginiPractice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportVinisha Vipin SharmaÎncă nu există evaluări
- Ceramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveDocument5 paginiCeramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveVinisha Vipin SharmaÎncă nu există evaluări
- Dentin HypersensitivityDocument62 paginiDentin HypersensitivityVinisha Vipin Sharma100% (1)
- Nanodentistry: New Buzz in Dentistry: Review ArticleDocument5 paginiNanodentistry: New Buzz in Dentistry: Review ArticleVinisha Vipin SharmaÎncă nu există evaluări
- PRISMA-P Statement - Moher Sys Rev Jan 2015Document9 paginiPRISMA-P Statement - Moher Sys Rev Jan 2015Vinisha Vipin SharmaÎncă nu există evaluări
- Esthetic Alternatives To AmalgamDocument15 paginiEsthetic Alternatives To AmalgamVinisha Vipin SharmaÎncă nu există evaluări
- Pin Retained RestorationDocument31 paginiPin Retained RestorationVinisha Vipin SharmaÎncă nu există evaluări
- Elements of MorphologyDocument16 paginiElements of MorphologySyrk12Încă nu există evaluări
- ABASII Sample Report F Hr2Document60 paginiABASII Sample Report F Hr2kalla55100% (1)
- Genital HerpesDocument2 paginiGenital HerpesWisnu WardanaÎncă nu există evaluări
- Composition of Blood and Cellular Elements: Learning ObjectivesDocument11 paginiComposition of Blood and Cellular Elements: Learning Objectivesmarinak_6Încă nu există evaluări
- Complete CPITN PRESENTATION PDFDocument16 paginiComplete CPITN PRESENTATION PDFThái ThịnhÎncă nu există evaluări
- Restraint CompetencyDocument6 paginiRestraint CompetencyFrederick RyanÎncă nu există evaluări
- Anaesthesiology NAGY TESZTKÖNYVDocument1.064 paginiAnaesthesiology NAGY TESZTKÖNYVoroszgabor100% (10)
- Intensive Revision Course in Paediatrics (Poster)Document2 paginiIntensive Revision Course in Paediatrics (Poster)Chris Jardine LiÎncă nu există evaluări
- FORM LPLPO & Permintaan TRIBULANDocument640 paginiFORM LPLPO & Permintaan TRIBULANMARTINIÎncă nu există evaluări
- Spinal Trauma, Imaging, Diagnosis and Management PDFDocument1 paginăSpinal Trauma, Imaging, Diagnosis and Management PDFskeithÎncă nu există evaluări
- Aditya MotwaneDocument3 paginiAditya Motwaneapi-257938623Încă nu există evaluări
- MCQ's With KEY Medicine - BDocument8 paginiMCQ's With KEY Medicine - BSiraj Ul IslamÎncă nu există evaluări
- Papp 2015 PFTDocument30 paginiPapp 2015 PFTWivina Bancoro100% (1)
- Antiparasitic DrugsDocument8 paginiAntiparasitic DrugsAdelina MariaÎncă nu există evaluări
- Leveling and AligningDocument21 paginiLeveling and AligningTatsanee Tanglitanont100% (5)
- E Book Mud Therapy TheoryDocument1 paginăE Book Mud Therapy Theoryvinda astri permatasariÎncă nu există evaluări
- High Risk PregnanciesDocument27 paginiHigh Risk PregnanciesMochammad Adam EldiÎncă nu există evaluări
- Emergency NursingDocument16 paginiEmergency NursingMandy Jamero100% (1)
- OSOM Regs 08Document12 paginiOSOM Regs 08Aymen ElatrashÎncă nu există evaluări
- Mortality RateDocument5 paginiMortality Rateamit kumar dewanganÎncă nu există evaluări
- Scapular Dyskinesis Increases The Risk of Future Shoulder Pain by 43% in Asymptomatic Athletes A Systematic Reviwer Nad Meta AnalysisDocument11 paginiScapular Dyskinesis Increases The Risk of Future Shoulder Pain by 43% in Asymptomatic Athletes A Systematic Reviwer Nad Meta AnalysisCesar C SÎncă nu există evaluări
- HLH BloodDocument13 paginiHLH BloodOmyRojasÎncă nu există evaluări
- MiracleDocument11 paginiMiracleJonatasCostaÎncă nu există evaluări
- Leggett Announces County Suit Against 14 Opioid CompaniesDocument163 paginiLeggett Announces County Suit Against 14 Opioid CompaniesPublic Information OfficeÎncă nu există evaluări
- Pocketbookofobstetricneonatalnpediatricemergencies PDFDocument378 paginiPocketbookofobstetricneonatalnpediatricemergencies PDFDANAÎncă nu există evaluări
- StahleDocument12 paginiStahlekhaledazima0% (2)
- Griffith 1898 PlatesDocument180 paginiGriffith 1898 PlateshaleliÎncă nu există evaluări
- Oral Physiology ReviewerDocument20 paginiOral Physiology ReviewerCamille Baybay100% (1)
- Practice Midterm Animal PhysDocument12 paginiPractice Midterm Animal Physrk0% (3)
- Femas Adetya Laudry - 22323052 - Tugas Bahasa Inggris Week 10Document8 paginiFemas Adetya Laudry - 22323052 - Tugas Bahasa Inggris Week 10asfem9935Încă nu există evaluări