S-ar putea să vă placă și
- The Little Lungs Book: Halting the march towards asthmaDe la EverandThe Little Lungs Book: Halting the march towards asthmaÎncă nu există evaluări
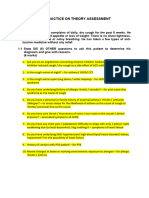
- CASE SIMUlation 112Document6 paginiCASE SIMUlation 112Princess Levie CenizaÎncă nu există evaluări
- The Whole Body Approach to Allergy and Sinus HealthDe la EverandThe Whole Body Approach to Allergy and Sinus HealthÎncă nu există evaluări
- PEDIA RLE Multiple Case Studies - 2Document4 paginiPEDIA RLE Multiple Case Studies - 2R-Chian Jose GermanpÎncă nu există evaluări
- The Asthma and Allergy Action Plan for Kids: A Complete Program to Help Your Child Live a Full and Active LifeDe la EverandThe Asthma and Allergy Action Plan for Kids: A Complete Program to Help Your Child Live a Full and Active LifeÎncă nu există evaluări
- Ped Paper CaseDocument9 paginiPed Paper CaseImmah PinedaÎncă nu există evaluări
- Care PlanDocument4 paginiCare PlangopscharanÎncă nu există evaluări
- 03 PAEDS NeurologyDocument13 pagini03 PAEDS Neurologyfire_n_iceÎncă nu există evaluări
- AntibioticDocument5 paginiAntibioticTumon HazarikaÎncă nu există evaluări
- Medicine CompleteDocument93 paginiMedicine CompletefdjslajfÎncă nu există evaluări
- Don't Let Asthma Steal Your Sleep: Feline FoeDocument4 paginiDon't Let Asthma Steal Your Sleep: Feline FoeAllergic Living magazineÎncă nu există evaluări
- IMCI Nov 2009Document141 paginiIMCI Nov 2009togononkaye100% (1)
- Marquez - Case Study 4Document4 paginiMarquez - Case Study 4Caren MarquezÎncă nu există evaluări
- Case Simulation 112 NNNNNNDocument5 paginiCase Simulation 112 NNNNNNLuiezt BernardoÎncă nu există evaluări
- Pedia Module Preschooler NeriDocument7 paginiPedia Module Preschooler NeriMantilla, Kristina Cassandra A.Încă nu există evaluări
- Alt To Ear Pain-1Document5 paginiAlt To Ear Pain-1nonoÎncă nu există evaluări
- BORLAND D. M., Homeopathy For Mother and Infant (Bl5)Document29 paginiBORLAND D. M., Homeopathy For Mother and Infant (Bl5)asyabatool100% (1)
- Case Study of Bronchial Asthma in Acute ExacerbationDocument16 paginiCase Study of Bronchial Asthma in Acute Exacerbationdextroid1290% (29)
- Cough, Pediatric: What Are The Causes?Document2 paginiCough, Pediatric: What Are The Causes?astarimediantoÎncă nu există evaluări
- Allergic Reaction To HomeworkDocument7 paginiAllergic Reaction To Homeworkh4aaj580100% (1)
- A Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Document13 paginiA Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Samantha BolanteÎncă nu există evaluări
- Health Care of The Pre School ChildDocument7 paginiHealth Care of The Pre School Childruthamerika6Încă nu există evaluări
- Pediatric AsthmaDocument63 paginiPediatric Asthmasrober0565Încă nu există evaluări
- Episodic SOAP Note Template - RX PedsDocument11 paginiEpisodic SOAP Note Template - RX PedsBrianne Foster75% (4)
- Imci Cough or DobDocument11 paginiImci Cough or DobRenz Jian MacasiebÎncă nu există evaluări
- Imci Case StudyDocument10 paginiImci Case StudyRhika Mae Flores Valdez100% (1)
- Respiratory Distress Case ScenarioDocument23 paginiRespiratory Distress Case ScenarioRakeesh VeeraÎncă nu există evaluări
- Condition 136 Fever, Irritability, Ear Discharge: TasksDocument2 paginiCondition 136 Fever, Irritability, Ear Discharge: Tasksmohamed aissaÎncă nu există evaluări
- Integrated Management On Childhood Illnesses 0101Document132 paginiIntegrated Management On Childhood Illnesses 0101James Felix Gallano Gales100% (1)
- Asthma Case Report FinalDocument6 paginiAsthma Case Report FinalJiaYee GoÎncă nu există evaluări
- Shelf Prep: Pediatric Patient NotesDocument9 paginiShelf Prep: Pediatric Patient NotesMaría Camila Pareja ZabalaÎncă nu există evaluări
- H'pathy-More Than A CureDocument106 paginiH'pathy-More Than A CureKrishna RathodÎncă nu există evaluări
- DANNY - RIVERA - MODIFIED VERSION - Episodic Visit TemplateDocument5 paginiDANNY - RIVERA - MODIFIED VERSION - Episodic Visit TemplateMallory ZaborÎncă nu există evaluări
- Prepared By: Ulfat Amin MSC Pediatric NursingDocument25 paginiPrepared By: Ulfat Amin MSC Pediatric NursingAngelic khanÎncă nu există evaluări
- Febrile Seizure Case FileDocument4 paginiFebrile Seizure Case Filehttps://medical-phd.blogspot.comÎncă nu există evaluări
- PC AssessmentDocument6 paginiPC AssessmentNabighah ZukriÎncă nu există evaluări
- Paediatrics - Febrile Convulsions Assessment, Treatment and Education PDFDocument12 paginiPaediatrics - Febrile Convulsions Assessment, Treatment and Education PDFPalash NagdeoteÎncă nu există evaluări
- TLC Noah HeerDocument3 paginiTLC Noah HeerAlain SalsaMan BazilÎncă nu există evaluări
- Case Study Form Tonsil It IsDocument3 paginiCase Study Form Tonsil It IsKayli EvansÎncă nu există evaluări
- IMCI - ContentDocument13 paginiIMCI - ContentMarianne Daphne GuevarraÎncă nu există evaluări
- Danny Rivera SOAPDocument4 paginiDanny Rivera SOAPariel sparkman100% (1)
- App To CHR CoughDocument6 paginiApp To CHR Coughbrajendra singhÎncă nu există evaluări
- Bicom For ChildrenDocument11 paginiBicom For ChildrenAnahata Fraydon100% (3)
- Untitled DocumentDocument42 paginiUntitled Documentallkhusairy6tuansiÎncă nu există evaluări
- Acute Otitis Media - 6435 SOAPDocument21 paginiAcute Otitis Media - 6435 SOAPMelinda Powell100% (1)
- Febrile SeizuresDocument6 paginiFebrile SeizuresKirstin del CarmenÎncă nu există evaluări
- Tonsillitis Information For ParentsDocument3 paginiTonsillitis Information For ParentsSalim JufriÎncă nu există evaluări
- Homoeopathy-More Than A Cure by Jiri CehovskyDocument107 paginiHomoeopathy-More Than A Cure by Jiri CehovskyHanah011011Încă nu există evaluări
- Soap Note 1Document3 paginiSoap Note 1Heather CunninghamÎncă nu există evaluări
- Otitis MediaDocument25 paginiOtitis Mediadmmwale1995Încă nu există evaluări
- Caridad C. Lintao, RN., Man School of Nursing Emilio Aguinaldo College - CaviteDocument32 paginiCaridad C. Lintao, RN., Man School of Nursing Emilio Aguinaldo College - CaviteImmanuel Capurcos Duabe JavilagÎncă nu există evaluări
- Management of A Patient With Lower Respiratory Tract DisordersDocument3 paginiManagement of A Patient With Lower Respiratory Tract DisordersCindy Mae de la TorreÎncă nu există evaluări
- What Is Mumps in ChildrenDocument4 paginiWhat Is Mumps in ChildrenFoster K KaundaÎncă nu există evaluări
- Module - Pre School PDFDocument11 paginiModule - Pre School PDFAnnaAlfonsoÎncă nu există evaluări
- Respiratory Conditions (Chapter 15) Flashcards - QuizletDocument4 paginiRespiratory Conditions (Chapter 15) Flashcards - QuizletEmily CallerÎncă nu există evaluări
- Module 13 - Common Childhood Illnesses - UpdatedDocument32 paginiModule 13 - Common Childhood Illnesses - UpdatedDIANA ACHEAMPONGÎncă nu există evaluări
- NCM109 RLE Assignment 1Document4 paginiNCM109 RLE Assignment 1Pollyn LazarteÎncă nu există evaluări
- Bronchiolitis ScriptDocument6 paginiBronchiolitis ScriptAhmed RmelahÎncă nu există evaluări
- Asthma - Child - Discharge: When You're in The HospitalDocument15 paginiAsthma - Child - Discharge: When You're in The HospitalJu Lie AnnÎncă nu există evaluări
- Micro para Laboratory Activity 4 - Case Study 2Document5 paginiMicro para Laboratory Activity 4 - Case Study 2Vannesa TarifaÎncă nu există evaluări
- Heat Stress ProcedureDocument13 paginiHeat Stress ProcedureKneekEy CastleÎncă nu există evaluări
- Slide IBSDocument34 paginiSlide IBSRamadhian Galih PratamaÎncă nu există evaluări
- Role of Ayurveda in Treating Cervical ErosionDocument9 paginiRole of Ayurveda in Treating Cervical Erosionrazvan rotaruÎncă nu există evaluări
- Acupuncture Modern MedicineDocument400 paginiAcupuncture Modern MedicineRoberto Biglia100% (5)
- Imaging in Transplantation PDFDocument259 paginiImaging in Transplantation PDFAnca MehedintuÎncă nu există evaluări
- Management of PcuDocument30 paginiManagement of Pcuapi-3698227Încă nu există evaluări
- CVVH Nel Post Operatorio Del Trapianto Di FegatoDocument5 paginiCVVH Nel Post Operatorio Del Trapianto Di FegatoMatteo BrambatiÎncă nu există evaluări
- 2 - EndometriosisDocument3 pagini2 - EndometriosisJayson Olile100% (1)
- Management of PPHDocument24 paginiManagement of PPHMutabazi SharifÎncă nu există evaluări
- Disease Signs & SymptomsDocument3 paginiDisease Signs & SymptomsJose Dangali AlinaoÎncă nu există evaluări
- Acl - Rehab - Protocol After Knee OperationDocument37 paginiAcl - Rehab - Protocol After Knee OperationGinoÎncă nu există evaluări
- Crick PrsentationDocument28 paginiCrick Prsentationalka mehraÎncă nu există evaluări
- 0226.OPWDD Letter From MembersDocument2 pagini0226.OPWDD Letter From MembersZacharyEJWilliamsÎncă nu există evaluări
- Headache and Joint PainDocument13 paginiHeadache and Joint PainJosiah Noella BrizÎncă nu există evaluări
- Unit 11 Introduction To EpidemiologyDocument38 paginiUnit 11 Introduction To EpidemiologyhumaÎncă nu există evaluări
- Fetal Biophysical ProfileDocument17 paginiFetal Biophysical ProfileBangun PurwakaÎncă nu există evaluări
- Nursing Skills (Vital Signs) PDFDocument48 paginiNursing Skills (Vital Signs) PDFkhizer hayatÎncă nu există evaluări
- Water HomeostasisDocument9 paginiWater HomeostasisRini MagfirahÎncă nu există evaluări
- 10 Dapat Tandaan Sa Pagsulat NG Artikulo Sa WikiFilipinoDocument2 pagini10 Dapat Tandaan Sa Pagsulat NG Artikulo Sa WikiFilipinoFrancisJudeRafilÎncă nu există evaluări
- امتحان سنة ثالثة 2023Document15 paginiامتحان سنة ثالثة 2023Dr-Mohammad Ali-Fayiz Al TamimiÎncă nu există evaluări
- Urban Inequities Survey ManualDocument364 paginiUrban Inequities Survey ManualAashishTripathiBaluaÎncă nu există evaluări
- Final PaperDocument58 paginiFinal PaperAngeline MirasolÎncă nu există evaluări
- Phylum PlatyhelminthesDocument19 paginiPhylum PlatyhelminthesBudi AfriyansyahÎncă nu există evaluări
- (EPEC) : Enteropathogenic E. ColiDocument1 pagină(EPEC) : Enteropathogenic E. ColiBig BearÎncă nu există evaluări
- Occupational Health Hazards Among Textile WorkersDocument9 paginiOccupational Health Hazards Among Textile WorkersINSTITUTE OF LEGAL EDUCATIONÎncă nu există evaluări
- Top 10 Differential Diagnoses in Family Medicine - CoughDocument2 paginiTop 10 Differential Diagnoses in Family Medicine - CoughTiza OyonÎncă nu există evaluări
- Table of Specification Mapeh 10Document4 paginiTable of Specification Mapeh 10Melody Anne Dinoso EvangelistaÎncă nu există evaluări
- Connective Tissue CellsDocument8 paginiConnective Tissue Cellsاسماء زياد عبدالجبارÎncă nu există evaluări
- 8 Heirs of Spouses Remedios R. Sandejas and Eliodoro P. Sandejas vs. LinaDocument9 pagini8 Heirs of Spouses Remedios R. Sandejas and Eliodoro P. Sandejas vs. LinaBerÎncă nu există evaluări
- CT Public v82 8 9Document2 paginiCT Public v82 8 9Dida HermaÎncă nu există evaluări
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)De la EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Evaluare: 3 din 5 stele3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 4.5 din 5 stele4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- Breaking the Habit of Being YourselfDe la EverandBreaking the Habit of Being YourselfEvaluare: 4.5 din 5 stele4.5/5 (1460)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 4 din 5 stele4/5 (4)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipDe la EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipEvaluare: 4.5 din 5 stele4.5/5 (1135)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDe la EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeEvaluare: 4.5 din 5 stele4.5/5 (254)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4.5 din 5 stele4.5/5 (6)
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingDe la EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingEvaluare: 4.5 din 5 stele4.5/5 (104)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingDe la EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingEvaluare: 4 din 5 stele4/5 (1138)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (170)