S-ar putea să vă placă și
- Florida Utility's Profit MaximizationDocument2 paginiFlorida Utility's Profit MaximizationAnonymous pvVCR5XLpÎncă nu există evaluări
- ENG104-GW-QUS - Summer2 - 2020 - OnlineDocument10 paginiENG104-GW-QUS - Summer2 - 2020 - OnlineAnonymous pvVCR5XLpÎncă nu există evaluări
- STELLA A Summer 2020Document6 paginiSTELLA A Summer 2020Anonymous pvVCR5XLpÎncă nu există evaluări
- Coursework 1Document4 paginiCoursework 1Anonymous pvVCR5XLpÎncă nu există evaluări
- Chapter 1&2Document15 paginiChapter 1&2Anonymous pvVCR5XLpÎncă nu există evaluări
- Fans Are Confused With The Kardashians' Most Recent Look: 'These Outfits Are The Ugliest'Document3 paginiFans Are Confused With The Kardashians' Most Recent Look: 'These Outfits Are The Ugliest'Anonymous pvVCR5XLpÎncă nu există evaluări
- Is Google Making Us Stupid EssayDocument5 paginiIs Google Making Us Stupid Essayapi-252844849100% (4)
- The Effects of Drug and Substance Abuse Among The Youth in United States - EditedDocument3 paginiThe Effects of Drug and Substance Abuse Among The Youth in United States - EditedAnonymous pvVCR5XLpÎncă nu există evaluări
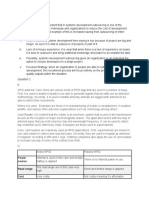
- RFID Antenna:: Power Source Read Range CostDocument2 paginiRFID Antenna:: Power Source Read Range CostAnonymous pvVCR5XLpÎncă nu există evaluări
- The Traits of LeadersDocument7 paginiThe Traits of LeadersAnonymous pvVCR5XLpÎncă nu există evaluări
- What Is China? Name University Tutor DateDocument7 paginiWhat Is China? Name University Tutor DateAnonymous pvVCR5XLpÎncă nu există evaluări
- Chapter 1&2Document4 paginiChapter 1&2Anonymous pvVCR5XLpÎncă nu există evaluări
- Divorce Analysis Name AffiliationDocument6 paginiDivorce Analysis Name AffiliationAnonymous pvVCR5XLpÎncă nu există evaluări
- Plagiarism Test 5 PDFDocument7 paginiPlagiarism Test 5 PDFAnonymous pvVCR5XLpÎncă nu există evaluări
- Starbuck SCM Name AffiliationDocument6 paginiStarbuck SCM Name AffiliationAnonymous pvVCR5XLpÎncă nu există evaluări
- Social Media Marketing PlanDocument62 paginiSocial Media Marketing PlanYannis A. PollalisÎncă nu există evaluări
- Types of Teams in Wells Fargo"Document1 paginăTypes of Teams in Wells Fargo"Anonymous pvVCR5XLpÎncă nu există evaluări
- Assignment DetailsDocument1 paginăAssignment DetailsAnonymous pvVCR5XLpÎncă nu există evaluări
- Types of Teams in Wells Fargo"Document1 paginăTypes of Teams in Wells Fargo"Anonymous pvVCR5XLpÎncă nu există evaluări
- Lesson 7 Case Study Yang Zheng International American University HC 510: Health Care and Law Ethics Prof. Muhammad Ashfaque February 18, 2018Document3 paginiLesson 7 Case Study Yang Zheng International American University HC 510: Health Care and Law Ethics Prof. Muhammad Ashfaque February 18, 2018Anonymous pvVCR5XLpÎncă nu există evaluări
- Effects of Global WarmingDocument1 paginăEffects of Global WarmingAnonymous pvVCR5XLpÎncă nu există evaluări
- Student's Name: Professor's Name: DateDocument5 paginiStudent's Name: Professor's Name: DateAnonymous pvVCR5XLpÎncă nu există evaluări
- TQM at Dubai HospitalDocument6 paginiTQM at Dubai HospitalAnonymous pvVCR5XLpÎncă nu există evaluări
- Untitled 1Document1 paginăUntitled 1Anonymous pvVCR5XLpÎncă nu există evaluări
- # 157850 Strategic Information SystemDocument12 pagini# 157850 Strategic Information SystemAnonymous pvVCR5XLpÎncă nu există evaluări
- Literary Analysis Pape..... OscarDocument17 paginiLiterary Analysis Pape..... OscarAnonymous pvVCR5XLpÎncă nu există evaluări
- Running Head: LESSON 3# CASE STUDIESDocument4 paginiRunning Head: LESSON 3# CASE STUDIESAnonymous pvVCR5XLpÎncă nu există evaluări
- Untitled DocumentDocument1 paginăUntitled DocumentAnonymous pvVCR5XLpÎncă nu există evaluări
- # 159753 Economics For Global DecisionDocument8 pagini# 159753 Economics For Global DecisionAnonymous pvVCR5XLpÎncă nu există evaluări
- Running Head: Organizational Governance and LeadershipDocument10 paginiRunning Head: Organizational Governance and LeadershipAnonymous pvVCR5XLpÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5782)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Heart of Arabia - A Record of Travel & ExplorationDocument503 paginiThe Heart of Arabia - A Record of Travel & ExplorationAltug100% (1)
- 10 Common Problems in The ClassroomDocument2 pagini10 Common Problems in The ClassroomNonnie CamporedondoÎncă nu există evaluări
- Queueing in The Linux Network StackDocument5 paginiQueueing in The Linux Network StackusakÎncă nu există evaluări
- The New York Times OppenheimerDocument3 paginiThe New York Times Oppenheimer徐大头Încă nu există evaluări
- Sovtek 5881 Wxt/6L6 WGC Tube GuideDocument8 paginiSovtek 5881 Wxt/6L6 WGC Tube GuideKon GekasÎncă nu există evaluări
- HST.582J / 6.555J / 16.456J Biomedical Signal and Image ProcessingDocument23 paginiHST.582J / 6.555J / 16.456J Biomedical Signal and Image ProcessingEduardo AlvarezÎncă nu există evaluări
- Magnesium Alloy Anodes For Cathodic ProtectionDocument2 paginiMagnesium Alloy Anodes For Cathodic Protectiongautam100% (1)
- HL Essay RubricDocument2 paginiHL Essay Rubricapi-520941535Încă nu există evaluări
- List of ISRO-DRDO JobsDocument2 paginiList of ISRO-DRDO Jobsjobkey.inÎncă nu există evaluări
- Green Schools Project LAC PlanDocument2 paginiGreen Schools Project LAC PlanJolly Mar Tabbaban Mangilaya100% (1)
- Speed Control of Brushless DC Motor Using Conventional ControllersDocument9 paginiSpeed Control of Brushless DC Motor Using Conventional ControllersMuhdnursalam ZolkepliÎncă nu există evaluări
- MEM - Project Pump and TurbineDocument22 paginiMEM - Project Pump and TurbineAbhi ChavanÎncă nu există evaluări
- Lista SindroameDocument28 paginiLista SindroameFeier CristianÎncă nu există evaluări
- Shariese-Moore-Resume NonumberDocument1 paginăShariese-Moore-Resume Nonumberapi-404271214Încă nu există evaluări
- Piaget'S Legacy As Reflected In: The Handbook of Child Psychology (1998 Edition)Document23 paginiPiaget'S Legacy As Reflected In: The Handbook of Child Psychology (1998 Edition)Melati SenjaÎncă nu există evaluări
- Amelia ResumeDocument3 paginiAmelia Resumeapi-305722904Încă nu există evaluări
- Finding Buyers Leather Footwear - Italy2Document5 paginiFinding Buyers Leather Footwear - Italy2Rohit KhareÎncă nu există evaluări
- Fiitjee Two Year Crp-2013-2015 Reshuffling Test - II Marks Test Date 30.03.2014Document35 paginiFiitjee Two Year Crp-2013-2015 Reshuffling Test - II Marks Test Date 30.03.2014Prateek__ManochaÎncă nu există evaluări
- Lewatit VP OC 1600 LDocument3 paginiLewatit VP OC 1600 Lphucuong2410Încă nu există evaluări
- Engrase SKF PDFDocument52 paginiEngrase SKF PDFTecnico AnzizarÎncă nu există evaluări
- LaSalle Network SurveyDocument23 paginiLaSalle Network SurveyAnonymous 6f8RIS6Încă nu există evaluări
- System ThinkingDocument18 paginiSystem Thinkingpptam50% (2)
- Lecture Nsche Engr Mafe SIWESDocument38 paginiLecture Nsche Engr Mafe SIWESoluomo1Încă nu există evaluări
- An Adaptive Memoryless Tag Anti-Collision Protocol For RFID NetworksDocument3 paginiAn Adaptive Memoryless Tag Anti-Collision Protocol For RFID Networkskinano123Încă nu există evaluări
- Reading SkillsDocument37 paginiReading SkillsShafinaz ZhumaÎncă nu există evaluări
- Maximum Mark: 50: Cambridge International ExaminationsDocument12 paginiMaximum Mark: 50: Cambridge International ExaminationsCanio100% (1)
- Aksel Yar: Syc-20360782#: :text Turner Syndrome, A Condition That, To D Evelop%Document4 paginiAksel Yar: Syc-20360782#: :text Turner Syndrome, A Condition That, To D Evelop%Mustafa Ayhan DuduÎncă nu există evaluări
- Khurda 2Document6 paginiKhurda 2papiraniÎncă nu există evaluări
- Fire Exit Doors SizeDocument3 paginiFire Exit Doors SizeBerlin Andrew SionÎncă nu există evaluări
- FET ExperimentDocument4 paginiFET ExperimentHayan FadhilÎncă nu există evaluări