S-ar putea să vă placă și
- The Acupuncture Prescription:: A Holistic Approach to HealthDe la EverandThe Acupuncture Prescription:: A Holistic Approach to HealthÎncă nu există evaluări
- Cranio em InglesDocument39 paginiCranio em InglesbrunamontenegrooÎncă nu există evaluări
- An Acupuncture Approach To Improved Breast HealthDocument1 paginăAn Acupuncture Approach To Improved Breast HealthmnaturaisÎncă nu există evaluări
- Home About Us Order Info FAQ Distributors Suppliers Feedback Contact Us View CartDocument5 paginiHome About Us Order Info FAQ Distributors Suppliers Feedback Contact Us View CartdpscribdzoneÎncă nu există evaluări
- What Is Laser Therapy?: How The Laser WorksDocument1 paginăWhat Is Laser Therapy?: How The Laser WorksvoxpapuliÎncă nu există evaluări
- Clinical Commentary On An Auricular Marker Associated With COVID-19Document2 paginiClinical Commentary On An Auricular Marker Associated With COVID-19yan92120Încă nu există evaluări
- 07 Caroline RadiceDocument7 pagini07 Caroline Radicetigerstyle1Încă nu există evaluări
- Acup Amenorrhea PDFDocument15 paginiAcup Amenorrhea PDFRonyÎncă nu există evaluări
- Where West Meets East: Traditional Asian MedicineDocument3 paginiWhere West Meets East: Traditional Asian MedicinesdASDdaÎncă nu există evaluări
- Tennis Elbow GetDocument20 paginiTennis Elbow GetHeri DwiantoÎncă nu există evaluări
- Balance Notes PDFDocument4 paginiBalance Notes PDFFarhan Ullah KhanÎncă nu există evaluări
- Massage Is An Intuitive Healing Art That Has Been Around For MillenniaDocument2 paginiMassage Is An Intuitive Healing Art That Has Been Around For MillenniaAjay Pal NattÎncă nu există evaluări
- Acupuntura y MenopausiaDocument10 paginiAcupuntura y MenopausiajesussalvadorsuazaÎncă nu există evaluări
- TCM Imassager Instruction Manual 2011.6Document24 paginiTCM Imassager Instruction Manual 2011.6drfaizal100% (1)
- Formulas MTCDocument13 paginiFormulas MTCSara RiosÎncă nu există evaluări
- Scalp Acupuncture AutismDocument2 paginiScalp Acupuncture AutismKoa Carlos CastroÎncă nu există evaluări
- Bioptron Colour 25Document34 paginiBioptron Colour 25diÎncă nu există evaluări
- The Effect of Microcurrents On Facial WrinklesDocument9 paginiThe Effect of Microcurrents On Facial WrinklesSofia RivaÎncă nu există evaluări
- WHO Standard Nomenclature of AcupunctureDocument36 paginiWHO Standard Nomenclature of AcupunctureTiffanny Anastasy100% (1)
- Ba Zhen Tang - 八珍湯 - Eight Treasures Decoction - Dang Gui and Ginseng Eight Combination - Chinese Herbs - American Dragon - Dr Joel Penner OMD, LAcDocument10 paginiBa Zhen Tang - 八珍湯 - Eight Treasures Decoction - Dang Gui and Ginseng Eight Combination - Chinese Herbs - American Dragon - Dr Joel Penner OMD, LAcangelesarenasÎncă nu există evaluări
- Acupressure Points Archives - Page 3 of 9 - Modern ReflexologyDocument30 paginiAcupressure Points Archives - Page 3 of 9 - Modern ReflexologyMiodrag Kolakovic100% (1)
- Acupuncture For The Treatment of Chronic Painful Peripheral Diabetic Neuropathy: A Long-Term StudyDocument7 paginiAcupuncture For The Treatment of Chronic Painful Peripheral Diabetic Neuropathy: A Long-Term StudyFernanda GiulianoÎncă nu există evaluări
- Japanese Scar TherapyDocument6 paginiJapanese Scar TherapyAngelaÎncă nu există evaluări
- Acupuncture Versus Opioids For Pain Relief: An Expert DiscussionDocument6 paginiAcupuncture Versus Opioids For Pain Relief: An Expert Discussionyan92120Încă nu există evaluări
- Tinnitus PresentationDocument16 paginiTinnitus PresentationScott MartinÎncă nu există evaluări
- Acupressure Training Course: Synopsis of Lesson IDocument2 paginiAcupressure Training Course: Synopsis of Lesson IAshishÎncă nu există evaluări
- Discover Instant and Natural Ways To Relieve Arthritis PainDe la EverandDiscover Instant and Natural Ways To Relieve Arthritis PainÎncă nu există evaluări
- Treating Facial Acne in Adolescents and Young Adults With Auriculoacupuncture and AuriculotherapyDocument16 paginiTreating Facial Acne in Adolescents and Young Adults With Auriculoacupuncture and AuriculotherapyPedro MaiaÎncă nu există evaluări
- Lecture+03+Chinese+Medicine+in+the+Late+Imperial+Period+Part+I +song Jin Yuan+STUDENTSDocument15 paginiLecture+03+Chinese+Medicine+in+the+Late+Imperial+Period+Part+I +song Jin Yuan+STUDENTSyuxi4417Încă nu există evaluări
- Microsystem NoteDocument18 paginiMicrosystem Noteyayanica100% (1)
- Connecting To CentreDocument4 paginiConnecting To CentreAna BarbaraÎncă nu există evaluări
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument18 paginiWorld's Largest Science, Technology & Medicine Open Access Book PublisherAndik SH100% (1)
- The Crossing Method of Point Selection: by DR Zhou Yu YanDocument3 paginiThe Crossing Method of Point Selection: by DR Zhou Yu YanJose Gregorio ParraÎncă nu există evaluări
- GlaucomaDocument6 paginiGlaucomaratamanoÎncă nu există evaluări
- A Skeptical Look at The AcuGraphDocument4 paginiA Skeptical Look at The AcuGraphhjsassoÎncă nu există evaluări
- Como Usar Las VentosasDocument4 paginiComo Usar Las VentosasMaritza Reds0% (1)
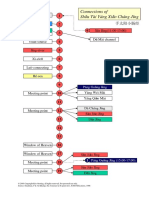
- Xiao Chang ConnectionsDocument1 paginăXiao Chang ConnectionspacdoxÎncă nu există evaluări
- The Leg Three Miles Acupuncture PointDocument5 paginiThe Leg Three Miles Acupuncture Pointdoktormin106Încă nu există evaluări
- Autonomic Regulation 1Document5 paginiAutonomic Regulation 1Darren StarwynnÎncă nu există evaluări
- Bhorn Fert LN TCMWTDocument10 paginiBhorn Fert LN TCMWTdrprasantÎncă nu există evaluări
- Bioptron Colour 38Document21 paginiBioptron Colour 38diÎncă nu există evaluări
- The Magic Touch The Simple Guide To Acupressure From Your Own Home 2157 7595.1000177Document4 paginiThe Magic Touch The Simple Guide To Acupressure From Your Own Home 2157 7595.1000177Haleelu Abdul JaleelÎncă nu există evaluări
- Summary of Chapter 11 of The Líng ShūDocument2 paginiSummary of Chapter 11 of The Líng ShūElanghovan ArumugamÎncă nu există evaluări
- 02-23 Kendall Mechanismofacupuncture FinalDocument3 pagini02-23 Kendall Mechanismofacupuncture FinalShahul Hameed100% (1)
- MT Fascia Poster 2 Final ImportanteDocument1 paginăMT Fascia Poster 2 Final ImportanteJessé de AndradeÎncă nu există evaluări
- M.E.a.D. Report ComparisonsDocument1 paginăM.E.a.D. Report ComparisonsFaisal MadjidÎncă nu există evaluări
- PPM May08 Kneebone LaserAcupunctureDocument4 paginiPPM May08 Kneebone LaserAcupuncturejoseÎncă nu există evaluări
- Ecto-Meso-Endo-Dermal LayersDocument3 paginiEcto-Meso-Endo-Dermal LayersCarissa NicholsÎncă nu există evaluări
- Test II-3.indd PDFDocument1 paginăTest II-3.indd PDFKika HadjÎncă nu există evaluări
- Acupressure and Su Jok PDFDocument5 paginiAcupressure and Su Jok PDFkholish najmuddinÎncă nu există evaluări
- What Is AcupunctureDocument3 paginiWhat Is AcupunctureSreedhar PulipatiÎncă nu există evaluări
- Prolonged Paroxysmal Sympathetic Storming Associated With Spontaneous Subarachnoid HemorrhageDocument5 paginiProlonged Paroxysmal Sympathetic Storming Associated With Spontaneous Subarachnoid Hemorrhageiri_balÎncă nu există evaluări
- The Acupressure Handbook: Ancient Healing Techniques for Today's WorldDe la EverandThe Acupressure Handbook: Ancient Healing Techniques for Today's WorldÎncă nu există evaluări
- Food for Thought: 25 Ways to Protect Yourself from Disease and Promote Excellent HealthDe la EverandFood for Thought: 25 Ways to Protect Yourself from Disease and Promote Excellent HealthÎncă nu există evaluări
- Chinese Herb Antagonists and IncompatibilitiesDocument2 paginiChinese Herb Antagonists and IncompatibilitiesbaihuguibanÎncă nu există evaluări
- Body Acupuncture For Nicotine Withdrawal Symptoms: A Randomized Placebo-Controlled TrialDocument6 paginiBody Acupuncture For Nicotine Withdrawal Symptoms: A Randomized Placebo-Controlled TrialGraziele GuimaraesÎncă nu există evaluări
- Acupuntura Protocolo Endometriose PDFDocument8 paginiAcupuntura Protocolo Endometriose PDFGraziele GuimaraesÎncă nu există evaluări
- Acupuntura Revisão SistemáticaDocument8 paginiAcupuntura Revisão SistemáticaGraziele GuimaraesÎncă nu există evaluări
- Workshop Policies: Joyce LowinsonDocument3 paginiWorkshop Policies: Joyce LowinsonGraziele GuimaraesÎncă nu există evaluări
- AA Efeito AntiinflamatórioDocument8 paginiAA Efeito AntiinflamatórioGraziele GuimaraesÎncă nu există evaluări
- Cor Pulmonale PATHOPHYSIOLOGYDocument2 paginiCor Pulmonale PATHOPHYSIOLOGYChloie Marie RosalejosÎncă nu există evaluări
- Gen EdDocument14 paginiGen EdMark Julius G AlmadinÎncă nu există evaluări
- Psychoactive Drugs ChartDocument5 paginiPsychoactive Drugs ChartAlessandra WilliamsÎncă nu există evaluări
- ABCDs During A Code Blue Response in An Adult PatientDocument23 paginiABCDs During A Code Blue Response in An Adult PatientChakra PuspitaÎncă nu există evaluări
- Vent Web HandoutDocument41 paginiVent Web Handoutwaqas_xsÎncă nu există evaluări
- Maternal Health: Ekta Modi 2 MPT in RehabDocument368 paginiMaternal Health: Ekta Modi 2 MPT in RehabMihir_Mehta_5497100% (1)
- HysterectomyDocument131 paginiHysterectomy8690402592Încă nu există evaluări
- CHN RLE Module 1M 3M With Self Assessment 1.2.3 of Rle Module 1mDocument62 paginiCHN RLE Module 1M 3M With Self Assessment 1.2.3 of Rle Module 1mPhilip Anthony Fernandez100% (1)
- MMC 8Document27 paginiMMC 8Neil Patrick AngelesÎncă nu există evaluări
- Methylmalonic and Propionic Acidemias: Clinical Management UpdateDocument25 paginiMethylmalonic and Propionic Acidemias: Clinical Management UpdateAnamarijaÎncă nu există evaluări
- Intra-Arterial Catheterization For Invasive Monitoring: Indications, Insertion Techniques, and Interpretation - UpToDateDocument40 paginiIntra-Arterial Catheterization For Invasive Monitoring: Indications, Insertion Techniques, and Interpretation - UpToDatejuanpbagurÎncă nu există evaluări
- K2 - Strongyloides StercoralisDocument16 paginiK2 - Strongyloides StercoraliswirputÎncă nu există evaluări
- Guide For Brachytherapy QA PDFDocument270 paginiGuide For Brachytherapy QA PDFtutorhowÎncă nu există evaluări
- Gold Awards: Organization Name Title of InnovationDocument10 paginiGold Awards: Organization Name Title of Innovationchek86351Încă nu există evaluări
- Scid 5 CVDocument26 paginiScid 5 CVZubair Mahmood KamalÎncă nu există evaluări
- Dental Hygiene Bab 15Document28 paginiDental Hygiene Bab 15Cinta SalsabilaÎncă nu există evaluări
- Nursing Care PlanDocument13 paginiNursing Care PlanJan DamesÎncă nu există evaluări
- Wadsworth Publishing Critical Reasoning 6thDocument468 paginiWadsworth Publishing Critical Reasoning 6thprabindra100% (1)
- CHON Lecture PDFDocument25 paginiCHON Lecture PDF2d HoehoeÎncă nu există evaluări
- Annotated Bibliography - Research ProjectDocument3 paginiAnnotated Bibliography - Research Projectapi-237847760Încă nu există evaluări
- Non - Food Meher Final Report (2023)Document87 paginiNon - Food Meher Final Report (2023)atakltigebertsadikÎncă nu există evaluări
- Rizal in DapitanDocument2 paginiRizal in DapitanMary Nicole PaedÎncă nu există evaluări
- FULL Download Ebook PDF Fundamentals of Human Neuropsychology 7th Edition PDF EbookDocument41 paginiFULL Download Ebook PDF Fundamentals of Human Neuropsychology 7th Edition PDF Ebookjennifer.lawver532100% (44)
- Gallstones: Session 4Document2 paginiGallstones: Session 4Valeria Casiano CelisÎncă nu există evaluări
- Covid-19 Detector Using The Power of Python and Arduino, This Detector Measures and Records User TemperatureDocument5 paginiCovid-19 Detector Using The Power of Python and Arduino, This Detector Measures and Records User TemperatureAshu SÎncă nu există evaluări
- Analgesics - New Microsoft Office Power Point PresentationDocument21 paginiAnalgesics - New Microsoft Office Power Point Presentationrozha100% (4)
- Nursing Care Plan Pott's DiseaseDocument2 paginiNursing Care Plan Pott's Diseasederic95% (21)
- Examination of ElbowDocument18 paginiExamination of Elbowharmohit singhÎncă nu există evaluări
- English Composition II 1Document11 paginiEnglish Composition II 1api-548473407Încă nu există evaluări
- Design Theory: Boo Virk Simon Andrews Boo - Virk@babraham - Ac.uk Simon - Andrews@babraham - Ac.ukDocument33 paginiDesign Theory: Boo Virk Simon Andrews Boo - Virk@babraham - Ac.uk Simon - Andrews@babraham - Ac.ukuzma munirÎncă nu există evaluări