S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- RWR WerwDocument1 paginăRWR WerwCélj Filmund GamayÎncă nu există evaluări
- Pyramid Con 320d Breaker Apr 2017Document2 paginiPyramid Con 320d Breaker Apr 2017Célj Filmund GamayÎncă nu există evaluări
- World Trends and Challenges 2016 GeneralDocument6 paginiWorld Trends and Challenges 2016 GeneralCélj Filmund GamayÎncă nu există evaluări
- 17-0066 Pyramid Con 320d Breaker Apr 2017Document3 pagini17-0066 Pyramid Con 320d Breaker Apr 2017Célj Filmund GamayÎncă nu există evaluări
- Credit Card Statement02Document1 paginăCredit Card Statement02Célj Filmund GamayÎncă nu există evaluări
- Donna J. Amoroso. New York and Oxford: Rowman and Littlefield Publishers, 2005. Softcover: 351ppDocument4 paginiDonna J. Amoroso. New York and Oxford: Rowman and Littlefield Publishers, 2005. Softcover: 351ppCélj Filmund GamayÎncă nu există evaluări
- DiaaazDocument2 paginiDiaaazCélj Filmund GamayÎncă nu există evaluări
- RizalDocument5 paginiRizalCélj Filmund GamayÎncă nu există evaluări
- Dela Cruz DanielaDocument15 paginiDela Cruz DanielaCélj Filmund GamayÎncă nu există evaluări
- FRUITEASDocument29 paginiFRUITEASCélj Filmund GamayÎncă nu există evaluări
- Tra VillaDocument6 paginiTra VillaCélj Filmund GamayÎncă nu există evaluări
- Mers-Cov Replicates in The Upper Respiratory Tracts of CamelsDocument2 paginiMers-Cov Replicates in The Upper Respiratory Tracts of CamelsCélj Filmund GamayÎncă nu există evaluări
- NovaDocument1 paginăNovaCélj Filmund GamayÎncă nu există evaluări
- Letter To The DeanDocument2 paginiLetter To The DeanCélj Filmund GamayÎncă nu există evaluări
- Memorandum of Agreement Between Laguindingan International Airport and Liceo de Cagayan University PartiesDocument2 paginiMemorandum of Agreement Between Laguindingan International Airport and Liceo de Cagayan University PartiesCélj Filmund GamayÎncă nu există evaluări
- Rizal Reflection NipangDocument3 paginiRizal Reflection NipangCélj Filmund GamayÎncă nu există evaluări
- Zest Two Oranges Using A ZesterDocument3 paginiZest Two Oranges Using A ZesterCélj Filmund GamayÎncă nu există evaluări
- Love Never Dies (Phantom of The Opera II)Document8 paginiLove Never Dies (Phantom of The Opera II)Célj Filmund GamayÎncă nu există evaluări
- The #Philippines Is A Nation of Starstruck Ignoramuses: Featured in Get Real PhilippinesDocument6 paginiThe #Philippines Is A Nation of Starstruck Ignoramuses: Featured in Get Real PhilippinesCélj Filmund GamayÎncă nu există evaluări
- Gamay, Celj Filmund B. Bsa - 4 AC-Comp 4 Mrs. Ana Maria S. CortesDocument2 paginiGamay, Celj Filmund B. Bsa - 4 AC-Comp 4 Mrs. Ana Maria S. CortesCélj Filmund GamayÎncă nu există evaluări
- Pmecpar FT AP InvestingDocument12 paginiPmecpar FT AP InvestingBryan JamesÎncă nu există evaluări
- Biology Major Tiffany Grace Uy Shared Some of Her Secrets After Finishing Summa Cum Laude in University of The Philippines DilimanDocument3 paginiBiology Major Tiffany Grace Uy Shared Some of Her Secrets After Finishing Summa Cum Laude in University of The Philippines DilimanCélj Filmund GamayÎncă nu există evaluări
- LGBT CommunityDocument10 paginiLGBT CommunityCélj Filmund GamayÎncă nu există evaluări
- Investments ProgramfdgfgfDocument30 paginiInvestments Programfdgfgfredearth2929Încă nu există evaluări
- Debate - Create A Logical ArgumentDocument11 paginiDebate - Create A Logical ArgumentCélj Filmund GamayÎncă nu există evaluări
- IRR AcadDocument20 paginiIRR AcadCélj Filmund GamayÎncă nu există evaluări
- MilitantDocument14 paginiMilitantCélj Filmund GamayÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Croup Diagnosis and Management 2018Document6 paginiCroup Diagnosis and Management 2018Jose Fernando DiezÎncă nu există evaluări
- Journal June 2019 - Empowering Occupational Health Doctor Through The Occupational Safety and Health (Noise Exposure) Regulation 2019Document30 paginiJournal June 2019 - Empowering Occupational Health Doctor Through The Occupational Safety and Health (Noise Exposure) Regulation 2019Ir ComplicatedÎncă nu există evaluări
- Causes of Clubbing - Google SearchDocument1 paginăCauses of Clubbing - Google SearchSheikh AnsaÎncă nu există evaluări
- Anesthesiology MnemonicsDocument1 paginăAnesthesiology MnemonicsMartin Susanto, MD100% (3)
- Diabetes Advisor - A Medical Expert System For Diabetes ManagementDocument5 paginiDiabetes Advisor - A Medical Expert System For Diabetes ManagementPrincess LunieÎncă nu există evaluări
- Raw Milk For The HealthDocument7 paginiRaw Milk For The HealthviannikkkyÎncă nu există evaluări
- Reports Webdocs W0215 FAQ ESC V2Document12 paginiReports Webdocs W0215 FAQ ESC V2Mythily RÎncă nu există evaluări
- Cytology and Cytological TechniquesDocument29 paginiCytology and Cytological TechniquessafiÎncă nu există evaluări
- Unit 10Document22 paginiUnit 10hafizur rahmanÎncă nu există evaluări
- Group 2 Con 1b Le4 Ca2Document25 paginiGroup 2 Con 1b Le4 Ca2Allyza Trixia Joyce VillasotoÎncă nu există evaluări
- Group B-2 Operation Management ProjectDocument17 paginiGroup B-2 Operation Management Projectanksri07Încă nu există evaluări
- Location of First Aid Kit OnboardDocument1 paginăLocation of First Aid Kit OnboardLoyd Christian MoradaÎncă nu există evaluări
- Daftar PustakaDocument2 paginiDaftar PustakaIntania MairudiÎncă nu există evaluări
- Flabby Alveolar Ridges: A Modified Technique To Treat This Clinical ChallengeDocument4 paginiFlabby Alveolar Ridges: A Modified Technique To Treat This Clinical ChallengeammarkochiÎncă nu există evaluări
- 2016 Annual Meeting Preliminary ProgramDocument62 pagini2016 Annual Meeting Preliminary ProgramDrVijaya VasanthakumarÎncă nu există evaluări
- ENGLISH 7-Week3Document2 paginiENGLISH 7-Week3JERIZZA MAGNE PARAFINAÎncă nu există evaluări
- Aloe Socotrina - A Most Valuable Remedy in Need of RediscoveryDocument6 paginiAloe Socotrina - A Most Valuable Remedy in Need of Rediscoverykrishna2205Încă nu există evaluări
- 02 Review of LiteratureDocument8 pagini02 Review of LiteratureAnnapoorna SHÎncă nu există evaluări
- Chap 1&3Document51 paginiChap 1&3Lady DanielleÎncă nu există evaluări
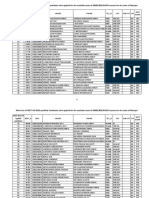
- Manipur Neet Ug Qualified Candidates ListDocument24 paginiManipur Neet Ug Qualified Candidates ListDenovo WangÎncă nu există evaluări
- PancitopeniasDocument34 paginiPancitopeniasJuan Pablo Fuentes ArriagadaÎncă nu există evaluări
- Concepts of Public HealthDocument8 paginiConcepts of Public Healtharn0ld21Încă nu există evaluări
- Guillain-Barre Syndrome: MSN 3 - Week 7A Ns. Lani Natalia Watania, M.KepDocument17 paginiGuillain-Barre Syndrome: MSN 3 - Week 7A Ns. Lani Natalia Watania, M.KepDevi100% (1)
- VVND TreatmentDocument4 paginiVVND Treatmentkarthivisu2009100% (1)
- Aetiology and Management of Tooth WearDocument13 paginiAetiology and Management of Tooth WearAravind KrishnanÎncă nu există evaluări
- Biological Properties of Lemongrass An OverviewDocument1 paginăBiological Properties of Lemongrass An OverviewLilia RotariÎncă nu există evaluări
- FilariasisDocument23 paginiFilariasisPrincess Gutierrez RositaÎncă nu există evaluări
- Epidemiology CourseworkDocument8 paginiEpidemiology Courseworkettgyrejd100% (2)
- Occupational Hazzards Affecting Healthcare ProffesionalsDocument17 paginiOccupational Hazzards Affecting Healthcare ProffesionalsMehnaz AbkrÎncă nu există evaluări
- Ally Treated Teeth As AbutmentsDocument6 paginiAlly Treated Teeth As AbutmentsLodi Al-SayedÎncă nu există evaluări