S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Ultimate Excel HandbookDocument43 paginiThe Ultimate Excel HandbookChandra RaoÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- "Red" High (1) "Yellow" Medium (2) "Green" Low (3) : IllnessDocument2 pagini"Red" High (1) "Yellow" Medium (2) "Green" Low (3) : IllnessBarb O'NeillÎncă nu există evaluări
- Jha RebarsDocument7 paginiJha RebarsJaycee QuinÎncă nu există evaluări
- ProcessSafetyManagement AuditApproachDocument8 paginiProcessSafetyManagement AuditApproachismailayarÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Guidelines For Hazard Evaluation Procedures 2nd Edition With Worked ExamplesDocument12 paginiGuidelines For Hazard Evaluation Procedures 2nd Edition With Worked Exampleskkkelvin21% (14)
- How To Build An Alcohol Distillation DeviceDocument45 paginiHow To Build An Alcohol Distillation Devicelokikg100% (2)
- NEOM-NPR-STD-001 - 01.00 Projects Health and Safety Assurance StandardDocument210 paginiNEOM-NPR-STD-001 - 01.00 Projects Health and Safety Assurance StandardHammad LiaqatÎncă nu există evaluări
- OSHAD-SF-TG-Laboratory Safety - V3.0 - EnglishDocument44 paginiOSHAD-SF-TG-Laboratory Safety - V3.0 - EnglishNiel Brian Villarazo0% (1)
- Is Audit Report 14489 (07-03-2018-122522)Document37 paginiIs Audit Report 14489 (07-03-2018-122522)Bhakti Mahbubani100% (4)
- Less Is MoreDocument16 paginiLess Is MoreismailayarÎncă nu există evaluări
- Method of Statement For SPI366 Pump Sump Cleaning Without Confined Space EntryDocument5 paginiMethod of Statement For SPI366 Pump Sump Cleaning Without Confined Space EntryKarpana Devi LetchumananÎncă nu există evaluări
- Powerwave ManagerDocument128 paginiPowerwave ManagerJackson Dias RochaÎncă nu există evaluări
- K To 12 CG - Agri-Crops - v1.0Document6 paginiK To 12 CG - Agri-Crops - v1.0may tagalogon villacoraÎncă nu există evaluări
- Balikpapan, April 17, 2007Document5 paginiBalikpapan, April 17, 2007Hasrul Sun100% (1)
- Moa For Work Immersion Lgu AnhsDocument7 paginiMoa For Work Immersion Lgu AnhsRechie Alaba LazalitaÎncă nu există evaluări
- En 14491-2006 Dust Explosion Venting Protective SystemsDocument32 paginiEn 14491-2006 Dust Explosion Venting Protective Systemsdmpresas100% (1)
- PL-3900 Battery Room Ventilation SystemDocument2 paginiPL-3900 Battery Room Ventilation SystemismailayarÎncă nu există evaluări
- UTS Dust Expl PrintDocument19 paginiUTS Dust Expl PrintismailayarÎncă nu există evaluări
- Clean Energy Technology Observatory Renewable fuels-KJNA31292ENNDocument59 paginiClean Energy Technology Observatory Renewable fuels-KJNA31292ENNismailayarÎncă nu există evaluări
- 004Document2 pagini004ismailayarÎncă nu există evaluări
- Combustible Dust Webinar HandoutDocument57 paginiCombustible Dust Webinar HandoutismailayarÎncă nu există evaluări
- DB 01097Document4 paginiDB 01097ismailayarÎncă nu există evaluări
- D 08 Ae 73279641 e 471Document15 paginiD 08 Ae 73279641 e 471ismailayarÎncă nu există evaluări
- Combustible Dust Webinar HandoutDocument57 paginiCombustible Dust Webinar HandoutismailayarÎncă nu există evaluări
- ALOHA ExamplesDocument53 paginiALOHA ExamplesismailayarÎncă nu există evaluări
- 7977 CCPS Annual2013 Low - ResDocument25 pagini7977 CCPS Annual2013 Low - ResismailayarÎncă nu există evaluări
- HAZOP Analysis Training GuideDocument7 paginiHAZOP Analysis Training GuideismailayarÎncă nu există evaluări
- VinegarDocument8 paginiVinegarMing HanÎncă nu există evaluări
- Lecture 12Document26 paginiLecture 12ismailayarÎncă nu există evaluări
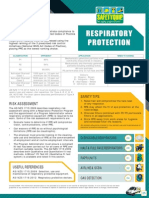
- RespiratoryprotectionDocument10 paginiRespiratoryprotectionismailayarÎncă nu există evaluări
- Free Cooling For Cooling TowersDocument28 paginiFree Cooling For Cooling TowersismailayarÎncă nu există evaluări
- 18537Document5 pagini18537ismailayarÎncă nu există evaluări
- Aiha Combustable DustsDocument47 paginiAiha Combustable DustsismailayarÎncă nu există evaluări
- Guidelines of Watermeter Installation 2009Document25 paginiGuidelines of Watermeter Installation 2009ismailayarÎncă nu există evaluări
- Iso HandbookDocument35 paginiIso Handbookrajeev_coralÎncă nu există evaluări
- Alcohol Fuel (Making Your Own)Document5 paginiAlcohol Fuel (Making Your Own)Alexandru MaximÎncă nu există evaluări
- Tutorial Ms AccessDocument15 paginiTutorial Ms AccessIka NovitasariÎncă nu există evaluări
- Flow Rate Measurements by FlumesDocument13 paginiFlow Rate Measurements by FlumesismailayarÎncă nu există evaluări
- AssessingRiskandControlling ExposureToPotentCompoundsDuringPackaging T&C May2010Document4 paginiAssessingRiskandControlling ExposureToPotentCompoundsDuringPackaging T&C May2010ismailayarÎncă nu există evaluări
- Hazard Analysis & Risk Modelling - InternationalDocument4 paginiHazard Analysis & Risk Modelling - Internationalaasimshaikh1110% (1)
- Primjer Testa Zaštite Na RaduDocument7 paginiPrimjer Testa Zaštite Na Radujelovina100% (1)
- Health, Safety & Environmental (HSE) Management System Audit QuestionsDocument26 paginiHealth, Safety & Environmental (HSE) Management System Audit QuestionsKalpana BansalÎncă nu există evaluări
- PROPASECDocument5 paginiPROPASECMeravigliorso76Încă nu există evaluări
- 427 Medical Assistant Associate DegreeDocument11 pagini427 Medical Assistant Associate DegreeSholida Depp-ReedusÎncă nu există evaluări
- Hierarchy of ControlsDocument2 paginiHierarchy of ControlsAbhash AryanÎncă nu există evaluări
- OSHMS360 Webinar COSH OutlineDocument4 paginiOSHMS360 Webinar COSH OutlineMichael NullasÎncă nu există evaluări
- MSDS - Degreasing Salt A - H+MDocument6 paginiMSDS - Degreasing Salt A - H+MAaed DahhamÎncă nu există evaluări
- Confined Space (Underfloor Entry)Document6 paginiConfined Space (Underfloor Entry)Tony ZhangÎncă nu există evaluări
- SM 3 PT Splitter Op ManDocument42 paginiSM 3 PT Splitter Op Manmanuel_plf0% (1)
- Lesson Plan in Afa8Document10 paginiLesson Plan in Afa8Maria Daisy ReyesÎncă nu există evaluări
- Safety Data Sheet GreaseDocument7 paginiSafety Data Sheet GreaseBurak YILMAZÎncă nu există evaluări
- Attachment 6 Job Observation / Task AnalysisDocument6 paginiAttachment 6 Job Observation / Task AnalysissaraÎncă nu există evaluări
- Pamphlet On Anti Termite Treatment PDFDocument4 paginiPamphlet On Anti Termite Treatment PDFCivil Site 17Încă nu există evaluări
- k3) Luxatherm5600 7954Document2 paginik3) Luxatherm5600 7954Syed FaridÎncă nu există evaluări
- # 110 Change Pump ModuleDocument1 pagină# 110 Change Pump ModuleHSE ManagerÎncă nu există evaluări
- Nitofill WS60: Uses PropertiesDocument4 paginiNitofill WS60: Uses PropertiesVenkata RaoÎncă nu există evaluări
- Nitrocellulose Hazardous SubstanceDocument6 paginiNitrocellulose Hazardous SubstanceoviangÎncă nu există evaluări
- IGC-3 Full AssessmentDocument13 paginiIGC-3 Full AssessmentMuhammad100% (1)
- Hilly Area ProcedureDocument59 paginiHilly Area ProcedurejohnÎncă nu există evaluări