S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Mccarthy Michael Et Al Touchstone 4 Teacher S Book PDFDocument253 paginiMccarthy Michael Et Al Touchstone 4 Teacher S Book PDFDain Mun75% (36)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Understanding God's Grace and Sin through a Child-Inclusive Sacramental TheologyDocument2 paginiUnderstanding God's Grace and Sin through a Child-Inclusive Sacramental TheologyPaul Lawrence100% (1)
- Variabel ASI EksklusifDocument6 paginiVariabel ASI EksklusifjumiyantiÎncă nu există evaluări
- Jurnal Self Excercise (Hemodialisis)Document8 paginiJurnal Self Excercise (Hemodialisis)Sebut Saja MawarÎncă nu există evaluări
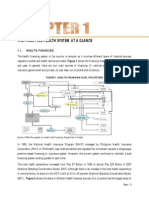
- Philippines health system overview: financing, facilities, human resourcesDocument15 paginiPhilippines health system overview: financing, facilities, human resourcesYL LYÎncă nu există evaluări
- AbstractDocument11 paginiAbstractjumiyantiÎncă nu există evaluări
- Chapter IVDocument80 paginiChapter IVjumiyantiÎncă nu există evaluări
- Review of Related LiteratureDocument56 paginiReview of Related LiteratureEka Sapta DesiyanaÎncă nu există evaluări
- Penge Sah AnDocument13 paginiPenge Sah AnEka Sapta DesiyanaÎncă nu există evaluări
- Chapter IVDocument80 paginiChapter IVjumiyantiÎncă nu există evaluări
- Chapter V ADocument18 paginiChapter V AEka Sapta DesiyanaÎncă nu există evaluări
- The Philippine Health Care Delivery SystemDocument7 paginiThe Philippine Health Care Delivery SystemJoselene Arenas DeDios95% (41)
- The Philippine Health Care Delivery SystemDocument7 paginiThe Philippine Health Care Delivery SystemJoselene Arenas DeDios95% (41)
- Philippines health system overview: financing, facilities, human resourcesDocument15 paginiPhilippines health system overview: financing, facilities, human resourcesYL LYÎncă nu există evaluări
- AbstractDocument11 paginiAbstractjumiyantiÎncă nu există evaluări
- Chapter V ADocument18 paginiChapter V AEka Sapta DesiyanaÎncă nu există evaluări
- OpenVetJ 5 18Document5 paginiOpenVetJ 5 18jumiyantiÎncă nu există evaluări
- Pone 0128964Document16 paginiPone 0128964jumiyantiÎncă nu există evaluări
- Chapter IDocument14 paginiChapter IjumiyantiÎncă nu există evaluări
- OpenVetJ 5 18Document5 paginiOpenVetJ 5 18jumiyantiÎncă nu există evaluări
- Pone 0128964Document16 paginiPone 0128964jumiyantiÎncă nu există evaluări
- Brmedj05811 0030aDocument1 paginăBrmedj05811 0030ajumiyantiÎncă nu există evaluări
- 448 877 1 SMDocument6 pagini448 877 1 SMWhira CahbaliÎncă nu există evaluări
- Hubungan Antara Hygiene Perorangan Dan Lingkungan Dengan Kejadian PiodermaDocument7 paginiHubungan Antara Hygiene Perorangan Dan Lingkungan Dengan Kejadian Piodermacute_chooeyÎncă nu există evaluări
- Hubungan Antara Hygiene Perorangan Dan Lingkungan Dengan Kejadian PiodermaDocument7 paginiHubungan Antara Hygiene Perorangan Dan Lingkungan Dengan Kejadian Piodermacute_chooeyÎncă nu există evaluări
- Innovativeness and Capacity To Innovate in A Complexity of Firm-Level Relationships A Response To WoodsideDocument3 paginiInnovativeness and Capacity To Innovate in A Complexity of Firm-Level Relationships A Response To Woodsideapi-3851548Încă nu există evaluări
- Ladder paradox resolved by relativity of simultaneityDocument11 paginiLadder paradox resolved by relativity of simultaneityperception888Încă nu există evaluări
- Subject: Social Studies Grade: 8 Topic: Understanding Worldview MaterialsDocument10 paginiSubject: Social Studies Grade: 8 Topic: Understanding Worldview Materialsapi-390372317Încă nu există evaluări
- Spread SstenoDocument37 paginiSpread SstenokanchanÎncă nu există evaluări
- The Thorny Way of Truth Part6 MarinovDocument332 paginiThe Thorny Way of Truth Part6 MarinovEvaldas StankeviciusÎncă nu există evaluări
- 165 - Shaking Hands Between Men WomenDocument9 pagini165 - Shaking Hands Between Men WomensakibpathanÎncă nu există evaluări
- Immigrant Women and Domestic Violence Common Experiences in Different CountriesDocument24 paginiImmigrant Women and Domestic Violence Common Experiences in Different Countriesapi-283710903100% (1)
- Right To Housing ArticleDocument32 paginiRight To Housing Articleapi-3743218Încă nu există evaluări
- Bar - Bar Waiter-EssDocument3 paginiBar - Bar Waiter-EssSebastia Felipe SolisÎncă nu există evaluări
- Persian 3 Minute Kobo AudiobookDocument194 paginiPersian 3 Minute Kobo AudiobookslojnotakÎncă nu există evaluări
- Explore India's Rich Literary HeritageDocument16 paginiExplore India's Rich Literary HeritageVipin MohanÎncă nu există evaluări
- Reading Comprehension Exercise # 211Document2 paginiReading Comprehension Exercise # 211Nuria CabreraÎncă nu există evaluări
- 13 Comedy StructuresDocument13 pagini13 Comedy Structuresrholzhauser01100% (6)
- Kanarev Photon Final PDFDocument12 paginiKanarev Photon Final PDFMaiman LatoÎncă nu există evaluări
- The Program For Better VisionDocument223 paginiThe Program For Better VisionBlasa100% (6)
- Part 3 Ready To PrintDocument18 paginiPart 3 Ready To Printjayrald cruzadaÎncă nu există evaluări
- Introductory Concepts and Definitions: Dr. Codruta Gosa Codruta - Gosa@e-UvtDocument15 paginiIntroductory Concepts and Definitions: Dr. Codruta Gosa Codruta - Gosa@e-UvtMădălina TodincaÎncă nu există evaluări
- High school years shape our futureDocument2 paginiHigh school years shape our futureSilva SharphyÎncă nu există evaluări
- Modern Business TemplatesDocument21 paginiModern Business TemplatesAntonio OtazúÎncă nu există evaluări
- Bringing Computational Thinking To STEM Education PDFDocument6 paginiBringing Computational Thinking To STEM Education PDFAkhy Syamsudin Al-fatihÎncă nu există evaluări
- 2012 PhenomenaDocument17 pagini2012 PhenomenaInderdip ShereÎncă nu există evaluări
- Hansel and Gretel Lit CritDocument11 paginiHansel and Gretel Lit Critdanica graceÎncă nu există evaluări
- Analyzing Learning Tasks & ObjectivesDocument9 paginiAnalyzing Learning Tasks & ObjectivesBeatrix Silvio Siregar SiloÎncă nu există evaluări
- Letterhead of OrganizationDocument3 paginiLetterhead of OrganizationeyoÎncă nu există evaluări
- Self Knowledge Self DisciplineDocument320 paginiSelf Knowledge Self DisciplineJose Kouassi88% (8)
- Terminal Performance Objective: A Detailed Lesson Plan in English For Grade 8 I. ObjectivesDocument12 paginiTerminal Performance Objective: A Detailed Lesson Plan in English For Grade 8 I. ObjectivesEdgar Gante Jr.Încă nu există evaluări
- ManagementDocument16 paginiManagementSahar Al-JoburyÎncă nu există evaluări
- The Modern Corsair Issue #3Document35 paginiThe Modern Corsair Issue #3TheModernCorsair100% (2)