S-ar putea să vă placă și
- Hemangiomas, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandHemangiomas, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Ranula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandRanula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
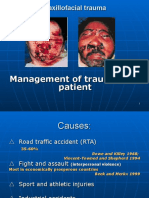
- Primary Management of Maxillofacial TraumaDocument34 paginiPrimary Management of Maxillofacial TraumafitsumÎncă nu există evaluări
- 1200 Walker MelissaDocument55 pagini1200 Walker Melissazano_adamÎncă nu există evaluări
- Benign Odontogenic Tumors of Jaws (AmeloblastomaDocument70 paginiBenign Odontogenic Tumors of Jaws (Ameloblastomagalina poberezhnikÎncă nu există evaluări
- Dentigerous Cyst: A Retrospective Study of 20 Cases in S. S. Medical College Rewa, Madhya PradeshDocument4 paginiDentigerous Cyst: A Retrospective Study of 20 Cases in S. S. Medical College Rewa, Madhya PradeshnjmdrÎncă nu există evaluări
- Erythema MultiformeDocument3 paginiErythema MultiformeLindar Rin リンÎncă nu există evaluări
- Ameloblastoma: Notorious Tumor of The Jaw - Report of A CaseDocument3 paginiAmeloblastoma: Notorious Tumor of The Jaw - Report of A CaseUwie MoumootÎncă nu există evaluări
- Unicystic Ameloblastoma of The Mandible - An Unusual Case Report and Review of LiteratureDocument5 paginiUnicystic Ameloblastoma of The Mandible - An Unusual Case Report and Review of LiteratureChristian Ivan SantosoÎncă nu există evaluări
- Oral and Maxillofacial Surgery Cases: Emtenan Abdulrahmman Almajid, Alia Khalid AlfadhelDocument5 paginiOral and Maxillofacial Surgery Cases: Emtenan Abdulrahmman Almajid, Alia Khalid AlfadhelAmadea EmanuelaÎncă nu există evaluări
- Radiographic Tumors PDFDocument58 paginiRadiographic Tumors PDFRiskha Febriani HapsariÎncă nu există evaluări
- Erythema Multiforme-Oral Variant: Case Report and Review of LiteratureDocument4 paginiErythema Multiforme-Oral Variant: Case Report and Review of LiteratureMarniati JohanÎncă nu există evaluări
- Desmoplastic Ameloblastoma of Anterior Mandible: Case Report of A RarityDocument5 paginiDesmoplastic Ameloblastoma of Anterior Mandible: Case Report of A RarityBimalKrishnaÎncă nu există evaluări
- Recent Advances in Diagnostic Oral MedicineDocument6 paginiRecent Advances in Diagnostic Oral Medicinegayathrireddy varikutiÎncă nu există evaluări
- Dr. Yoseph - The Role of Radiotherapy in The Management of Ameloblastoma and Ameloblastic CarcinomaDocument10 paginiDr. Yoseph - The Role of Radiotherapy in The Management of Ameloblastoma and Ameloblastic CarcinomaOnkologi Radiasi Angkatan 23Încă nu există evaluări
- Scleroderma - A Case ReportDocument3 paginiScleroderma - A Case Reportdhea nadhiaÎncă nu există evaluări
- Bitewing and Occlusal 2021Document47 paginiBitewing and Occlusal 2021Khadyjah RashidÎncă nu există evaluări
- Oral Mucositis-A Sequal To Cancer Therapy-Prevention and ManagementDocument3 paginiOral Mucositis-A Sequal To Cancer Therapy-Prevention and Managementumerjaved86Încă nu există evaluări
- Management of Oral Leukoplakia - Analysis of The Literature: Material and MethodsDocument10 paginiManagement of Oral Leukoplakia - Analysis of The Literature: Material and MethodsyunisaÎncă nu există evaluări
- Angina LudwigDocument4 paginiAngina LudwigArri KurniawanÎncă nu există evaluări
- Molecular Etiopathogenesis of Ameloblastoma CurrentDocument5 paginiMolecular Etiopathogenesis of Ameloblastoma CurrentRiskha Febriani HapsariÎncă nu există evaluări
- Case Report Redy-Histologic Variants of AmeloblastomaDocument6 paginiCase Report Redy-Histologic Variants of Ameloblastomariris roselinaÎncă nu există evaluări
- Muscle Examination With Middle 3 Fingers With 1-2 Second ThrustsDocument4 paginiMuscle Examination With Middle 3 Fingers With 1-2 Second ThrustsFahad QiamÎncă nu există evaluări
- Modul Wound Bed Preparation DR Ardianto SucintaDocument37 paginiModul Wound Bed Preparation DR Ardianto SucintaArdianto SucintaÎncă nu există evaluări
- Dr. Lakshmi Narayana Malabar Cancer CentreDocument81 paginiDr. Lakshmi Narayana Malabar Cancer Centresherani999Încă nu există evaluări
- Focal InfectionDocument6 paginiFocal InfectionDwi RahmaÎncă nu există evaluări
- Salivary Gland RadiologyDocument110 paginiSalivary Gland RadiologyHeba S RadaidehÎncă nu există evaluări
- Gerodontology BaruDocument53 paginiGerodontology BaruHappy Septianto S100% (1)
- Unicystic AmeloblastomaDocument5 paginiUnicystic AmeloblastomaayuÎncă nu există evaluări
- An Overview of Burning Mouth SyndromeDocument10 paginiAn Overview of Burning Mouth SyndromerosaÎncă nu există evaluări
- Recurrent Herpes LabialisDocument25 paginiRecurrent Herpes LabialisGarry B GunawanÎncă nu există evaluări
- Department of Traumatology and Orthopedics BleedingDocument75 paginiDepartment of Traumatology and Orthopedics Bleedinglopez logeeÎncă nu există evaluări
- Bone Grafts, Bone Substitutes and OrthobiologicsDocument11 paginiBone Grafts, Bone Substitutes and Orthobiologicshaqqulmauludiyah_ict_ismkiÎncă nu există evaluări
- Trigeminal Neuralgia A Case Report With Review of LiteratureDocument4 paginiTrigeminal Neuralgia A Case Report With Review of LiteratureFauziah KautsaraÎncă nu există evaluări
- Bisphosphonate Related Osteonecrosis of The Jaw (Bronj)Document33 paginiBisphosphonate Related Osteonecrosis of The Jaw (Bronj)jazzy penzÎncă nu există evaluări
- Cleftlipandpalate 111008125422 Phpapp02Document81 paginiCleftlipandpalate 111008125422 Phpapp02samira fatimaÎncă nu există evaluări
- Fraktur Tulang: Husnul Author Bag. Bedah RSUD CilacapDocument26 paginiFraktur Tulang: Husnul Author Bag. Bedah RSUD CilacapUmi YatunÎncă nu există evaluări
- Mucositis GuidlinesDocument13 paginiMucositis GuidlinesEman MossanÎncă nu există evaluări
- Ludwigs Angina - Emergency TreatmentDocument3 paginiLudwigs Angina - Emergency TreatmentsorayahyuraÎncă nu există evaluări
- Referat Primery Bone TumorsDocument62 paginiReferat Primery Bone Tumorsrahma nilasari100% (1)
- Pressure Ulcer Prevention & Management: Wocare ClinicDocument20 paginiPressure Ulcer Prevention & Management: Wocare ClinicShoahir RustanÎncă nu există evaluări
- The Occlusal Splint TherapyDocument5 paginiThe Occlusal Splint TherapyVíctor Adolfo Ravelo SalinasÎncă nu există evaluări
- Dr. Ago Harlim - MikosisDocument50 paginiDr. Ago Harlim - MikosisBrian Pasa NababanÎncă nu există evaluări
- Rupture Tendon Digiti III, IV, V Manus Sinistra Vulnus Laceratum Wrist Joint SinistraDocument13 paginiRupture Tendon Digiti III, IV, V Manus Sinistra Vulnus Laceratum Wrist Joint SinistraNubhy NubÎncă nu există evaluări
- Acute Scrotum 231016 PDFDocument50 paginiAcute Scrotum 231016 PDFDany Dias100% (1)
- Diabetic UlcerDocument56 paginiDiabetic UlcermucfhsinÎncă nu există evaluări
- Retinopati DiabetikDocument5 paginiRetinopati DiabetikMuhammad Afriadi HamdanÎncă nu există evaluări
- Infeksi NosokomialDocument29 paginiInfeksi NosokomialAlunaficha Melody KiraniaÎncă nu există evaluări
- Eagle's Syndrome-15-07-2015 PDFDocument39 paginiEagle's Syndrome-15-07-2015 PDFfahriitoÎncă nu există evaluări
- Trismus - An Aetiology and ManagementDocument5 paginiTrismus - An Aetiology and ManagementNandakumar PargunanÎncă nu există evaluări
- Endodontic-Periodontal Lesion: A Two-Way Traffic: Dr. Anindya Priya Saha, Dr. Anindya Chakraborty and Dr. Sananda SahaDocument6 paginiEndodontic-Periodontal Lesion: A Two-Way Traffic: Dr. Anindya Priya Saha, Dr. Anindya Chakraborty and Dr. Sananda Sahanovia chantikaÎncă nu există evaluări
- TMJ DislocationDocument56 paginiTMJ DislocationAlok BhardwajÎncă nu există evaluări
- Case Report: Osteoarthritis: Mutiara Riahna Sitepu 030.12.179 Pembimbing Dr. T. Nurrobi, SP - OT (K) HandDocument50 paginiCase Report: Osteoarthritis: Mutiara Riahna Sitepu 030.12.179 Pembimbing Dr. T. Nurrobi, SP - OT (K) Handmutiara sitepuÎncă nu există evaluări
- CBCT Third Eye in Dental ImplantDocument24 paginiCBCT Third Eye in Dental ImplantNajeeb Ullah100% (1)
- Autoimmune Diseases of The Oral CavityDocument143 paginiAutoimmune Diseases of The Oral CavityMohammed ShaikhÎncă nu există evaluări
- Fraktur Humerus Sepertiga DistalDocument26 paginiFraktur Humerus Sepertiga DistalNurul Rezki Fitriani AzisÎncă nu există evaluări
- Anodontia of Permanent Teeth - A Case ReportDocument3 paginiAnodontia of Permanent Teeth - A Case Reportanandsingh001Încă nu există evaluări
- Leukoplakia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandLeukoplakia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Dermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaDe la EverandDermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaÎncă nu există evaluări
- TrismusDocument4 paginiTrismusEkaÎncă nu există evaluări
- AntiplateletDocument8 paginiAntiplateletAdityaEdoÎncă nu există evaluări
- CTS TreatmentDocument16 paginiCTS TreatmentAdityaEdoÎncă nu există evaluări
- AntiplateletDocument8 paginiAntiplateletAdityaEdoÎncă nu există evaluări
- Frozen ShoulderDocument5 paginiFrozen ShoulderAdityaEdoÎncă nu există evaluări
- 187 1 Li and Greenwall SafetyDocument6 pagini187 1 Li and Greenwall SafetydigdouwÎncă nu există evaluări
- Mucocutaneous Occurrences of The Syphilis in Pregnant and Hiv Positive WomenDocument4 paginiMucocutaneous Occurrences of The Syphilis in Pregnant and Hiv Positive WomenAdityaEdoÎncă nu există evaluări
- Benzathine Penicillin For Preventing SipilisDocument9 paginiBenzathine Penicillin For Preventing SipilisAdityaEdoÎncă nu există evaluări
- Antigen Kuantitatif NS1 Dan Keparahan Infeksi Virus DengueDocument4 paginiAntigen Kuantitatif NS1 Dan Keparahan Infeksi Virus DengueAdityaEdoÎncă nu există evaluări
- Syndromes Palmoplantar KeratodermaDocument6 paginiSyndromes Palmoplantar KeratodermaAdityaEdoÎncă nu există evaluări
- PneumoniaDocument24 paginiPneumoniaWidhi AstutiÎncă nu există evaluări
- Treatment of Infantile Capillary Hemangioma of TheDocument7 paginiTreatment of Infantile Capillary Hemangioma of TheAdityaEdoÎncă nu există evaluări
- Gambar Lowback PainDocument5 paginiGambar Lowback PainAdityaEdoÎncă nu există evaluări
- Cancer of LarynxDocument3 paginiCancer of LarynxShreyas WalvekarÎncă nu există evaluări
- Case Study Breast CaDocument32 paginiCase Study Breast Caapi-391376321Încă nu există evaluări
- 64 - Skin TumorsDocument20 pagini64 - Skin TumorsAlexa GabrielaÎncă nu există evaluări
- Literature Review On LeukemiaDocument8 paginiLiterature Review On Leukemiaafdtukasg100% (2)
- 4-Week UFAPS With FA 2021Document2 pagini4-Week UFAPS With FA 2021susannahshinyÎncă nu există evaluări
- World Congress of Internal Medicine (WCIM) 2014 Poster PresentationDocument34 paginiWorld Congress of Internal Medicine (WCIM) 2014 Poster PresentationTenri AshariÎncă nu există evaluări
- Test Bank For Wongs Essentials of Pediatric Nursing 7th Edition Marilyn J HockenberryDocument36 paginiTest Bank For Wongs Essentials of Pediatric Nursing 7th Edition Marilyn J Hockenberrypervaderubicundrulipp100% (37)
- European Association of UROLOGY Pocket Guidelines 2017Document416 paginiEuropean Association of UROLOGY Pocket Guidelines 2017Anonymous GwP922jlÎncă nu există evaluări
- World's Largest Medicineless HospitalDocument1 paginăWorld's Largest Medicineless HospitalTJ MzamokumalaÎncă nu există evaluări
- tp132 c2 PDFDocument9 paginitp132 c2 PDFAntonio C. KeithÎncă nu există evaluări
- Simu 20 Test 2Document108 paginiSimu 20 Test 2Profile Info100% (1)
- Biologia PlantelorDocument23 paginiBiologia PlantelorCristina Teodora BerbecaruÎncă nu există evaluări
- Medical TermDocument33 paginiMedical TermZahra PratiwiÎncă nu există evaluări
- Cervical Cancer ScreeningDocument25 paginiCervical Cancer Screening6ixSideCreate MÎncă nu există evaluări
- Cervical Cancer: Dr. Sushma DhakalDocument137 paginiCervical Cancer: Dr. Sushma DhakalBhattarai ShrinkhalaÎncă nu există evaluări
- Icccpo Newsletter 2006 01Document18 paginiIcccpo Newsletter 2006 01DIOGEN_2014Încă nu există evaluări
- Fda Approved Contrast AgentsDocument55 paginiFda Approved Contrast AgentsPoojaSolankiÎncă nu există evaluări
- Breast Examination - ADocument30 paginiBreast Examination - AAkash VermaÎncă nu există evaluări
- Crossroads Summer 08Document62 paginiCrossroads Summer 08jason.garber100% (4)
- Mike Adams - Secret Sources For Healing Foods and Natural MedicinesDocument67 paginiMike Adams - Secret Sources For Healing Foods and Natural MedicinesAnonymous 3YNFShC100% (3)
- Far Eastern University-Institute of Nursing In-House NursingDocument25 paginiFar Eastern University-Institute of Nursing In-House Nursingjonasdelacruz1111Încă nu există evaluări
- NP - Iv MSDocument96 paginiNP - Iv MSReyna Marie Labadan-Lasacar100% (1)
- Pathcare May-Aug PDFDocument6 paginiPathcare May-Aug PDFdenosciÎncă nu există evaluări
- Medical Oncology Maintenance of Certification Examination Blueprint - American Board of Internal MedicineDocument4 paginiMedical Oncology Maintenance of Certification Examination Blueprint - American Board of Internal MedicineabimorgÎncă nu există evaluări
- Scalp Tumors: CME ArticleDocument3 paginiScalp Tumors: CME Articlenailatul fadhilaÎncă nu există evaluări
- Urine TherapyDocument5 paginiUrine TherapyMichal SladekÎncă nu există evaluări
- Brain Tumors (Benign and Malignant) - Symptoms, Causes, TreatmentDocument4 paginiBrain Tumors (Benign and Malignant) - Symptoms, Causes, TreatmentThuvija DarshiniÎncă nu există evaluări
- Presentation2 BREAST IMAGING - LatestDocument53 paginiPresentation2 BREAST IMAGING - LatestLadipo Temitope AyodejiÎncă nu există evaluări
- InformaciónDocument14 paginiInformaciónAlondraÎncă nu există evaluări
- Power Against Breast Cancer Prayer 2013Document2 paginiPower Against Breast Cancer Prayer 2013John Arthur100% (1)