S-ar putea să vă placă și
- CCI Student ApplicationDocument4 paginiCCI Student ApplicationIbrahim KalokohÎncă nu există evaluări
- KwaZulu Natal Department of Transport Bursary Application FormDocument8 paginiKwaZulu Natal Department of Transport Bursary Application FormMandisa ZibulaÎncă nu există evaluări
- Personal Inventory Form Informatics Version 2Document3 paginiPersonal Inventory Form Informatics Version 2charles199326Încă nu există evaluări
- KZN COGTA Bursary Application Form 2024Document7 paginiKZN COGTA Bursary Application Form 2024thabisileÎncă nu există evaluări
- NJCAA Eligibility Affidavit: Personal InformationDocument2 paginiNJCAA Eligibility Affidavit: Personal InformationerronÎncă nu există evaluări
- Formulário - Allan MudhlovoDocument8 paginiFormulário - Allan MudhlovoJean MichelÎncă nu există evaluări
- Guidance Office Personal Data InventoryDocument16 paginiGuidance Office Personal Data InventoryCharlyn May Valenzuela SimonÎncă nu există evaluări
- St. Paul College Foundation, Inc. Health Services Department Referral Slip (Guidance CounselorDocument3 paginiSt. Paul College Foundation, Inc. Health Services Department Referral Slip (Guidance CounselorAnonymous g83dcTWÎncă nu există evaluări
- Hyde Square Task Force Youth Leadership ApplicationDocument9 paginiHyde Square Task Force Youth Leadership ApplicationKaren BossÎncă nu există evaluări
- C C J E: Student Information SheetDocument2 paginiC C J E: Student Information SheetBannuar kappia SagunÎncă nu există evaluări
- Ateneo de Zamboanga University: Application For Senior High School AdmissionDocument3 paginiAteneo de Zamboanga University: Application For Senior High School AdmissionAcel MonjardinÎncă nu există evaluări
- Opg SchoolDocument4 paginiOpg SchoolmirajulhaqÎncă nu există evaluări
- Brag SheetDocument1 paginăBrag Sheetapi-412826792Încă nu există evaluări
- Memorial Go-Kart Inc.: 5308 Hwy 175 Hartford, WI 53027 262-644-8375Document5 paginiMemorial Go-Kart Inc.: 5308 Hwy 175 Hartford, WI 53027 262-644-8375Hafiezul HassanÎncă nu există evaluări
- FEBC Info Sheet - NEWDocument5 paginiFEBC Info Sheet - NEWnigel alinsug0% (1)
- Sarvodaya Foundation Education Assistance FormDocument4 paginiSarvodaya Foundation Education Assistance FormJenish JobaliyaÎncă nu există evaluări
- Kami Export - Resume 1 2 2 1Document3 paginiKami Export - Resume 1 2 2 1api-693823232Încă nu există evaluări
- AppForm 11111HSDocument6 paginiAppForm 11111HSvainly4u8155Încă nu există evaluări
- BGLC Scholarship Application FormDocument5 paginiBGLC Scholarship Application FormVernon WhiteÎncă nu există evaluări
- Nyandarua BursaryAPPLICATION FORMDocument5 paginiNyandarua BursaryAPPLICATION FORMK Kamau100% (1)
- Bursary Application-FormDocument5 paginiBursary Application-FormPhelein David100% (1)
- Student Profile Form For Inventory - PDFDocument2 paginiStudent Profile Form For Inventory - PDFLeen Ganoran100% (1)
- DMSF College of Medicine ApplicationDocument4 paginiDMSF College of Medicine ApplicationJehannaMarEnggingAbdurahmanÎncă nu există evaluări
- Student Information SheetDocument3 paginiStudent Information SheetNojelyn VillanuevaÎncă nu există evaluări
- DMSF College of Medicine ApplicationDocument4 paginiDMSF College of Medicine ApplicationAlsalman AnamÎncă nu există evaluări
- Scholarship ApplicationDocument2 paginiScholarship ApplicationMVRUÎncă nu există evaluări
- Student profile formDocument2 paginiStudent profile formMichaelViloriaÎncă nu există evaluări
- Day On The Job PacketDocument11 paginiDay On The Job Packetapi-372716778Încă nu există evaluări
- Letter of Recommendation RequestDocument2 paginiLetter of Recommendation Requestapi-527944284Încă nu există evaluări
- College Cumulative Record 2x2 ID PictureDocument3 paginiCollege Cumulative Record 2x2 ID PictureraffiemarieÎncă nu există evaluări
- Distinction College-Application FormDocument2 paginiDistinction College-Application FormŠüprėmë DøńÎncă nu există evaluări
- Application For The 2010 Piedmont Chapter AFSDocument2 paginiApplication For The 2010 Piedmont Chapter AFSapi-26027356Încă nu există evaluări
- Student InventoryDocument2 paginiStudent Inventoryleo dumapiÎncă nu există evaluări
- General Scholarship Application Form: First LastDocument3 paginiGeneral Scholarship Application Form: First LastKen BiÎncă nu există evaluări
- Happiness Form For All Level I CoursesDocument1 paginăHappiness Form For All Level I CoursesRabin BhattaraiÎncă nu există evaluări
- Inquiry Form1Document2 paginiInquiry Form1ammuÎncă nu există evaluări
- Resident Leadership Program App Packet - Nov2018Document6 paginiResident Leadership Program App Packet - Nov2018Subhasis RoyÎncă nu există evaluări
- DMSF College of NursingApplicationDocument4 paginiDMSF College of NursingApplicationrodentÎncă nu există evaluări
- CbeapplicationformDocument3 paginiCbeapplicationformKemo JacksonÎncă nu există evaluări
- Empapp 2016 BDocument5 paginiEmpapp 2016 Bapi-393899350Încă nu există evaluări
- Johnny Q - Employment Application FormDocument3 paginiJohnny Q - Employment Application Formprettyboiricky54Încă nu există evaluări
- U.S. Counselling Profile FormDocument6 paginiU.S. Counselling Profile FormVamsi Krishna KvÎncă nu există evaluări
- Christian Life ProgramDocument1 paginăChristian Life ProgramGeleenÎncă nu există evaluări
- Buah Hati / Cita Hati School Buah Hati / Cita Hati School: Application For EmploymentDocument4 paginiBuah Hati / Cita Hati School Buah Hati / Cita Hati School: Application For EmploymentId Card AndreÎncă nu există evaluări
- Home Visitation Slip 2020 2021Document2 paginiHome Visitation Slip 2020 2021doreen ann montanoÎncă nu există evaluări
- Dr. Filemon C. Aguilar Memorial College of Las Piñas: GTI-FORM-012-2013Document2 paginiDr. Filemon C. Aguilar Memorial College of Las Piñas: GTI-FORM-012-2013Mary KimÎncă nu există evaluări
- Application FOR EmploymentDocument4 paginiApplication FOR Employment3187265Încă nu există evaluări
- Application GuideDocument6 paginiApplication GuidePem MianoÎncă nu există evaluări
- London Kids Admn Form - CDRDocument4 paginiLondon Kids Admn Form - CDRDeeniyat ChanserpurÎncă nu există evaluări
- HAU - Academic Counseling FormDocument1 paginăHAU - Academic Counseling FormBerlon LacsonÎncă nu există evaluări
- CCSHS FormDocument2 paginiCCSHS FormDzay RowlÎncă nu există evaluări
- Falcon Links Trsvels SND Tours: Application For AgancyDocument6 paginiFalcon Links Trsvels SND Tours: Application For AgancyKHAWAJAÎncă nu există evaluări
- FormDocument4 paginiFormAble K-HeavenÎncă nu există evaluări
- Info SheetDocument7 paginiInfo SheetALJON DONGALLOÎncă nu există evaluări
- Qat Form C 1Document3 paginiQat Form C 1Seanjames JacobÎncă nu există evaluări
- Request Letters RecDocument7 paginiRequest Letters RecCher Tùng VoÎncă nu există evaluări
- 15 Exercises On Resume WritingDocument38 pagini15 Exercises On Resume Writingangeline salongaÎncă nu există evaluări
- The Honest and Direct Truth to Resumes from an HR Director PerspectiveDe la EverandThe Honest and Direct Truth to Resumes from an HR Director PerspectiveÎncă nu există evaluări
- MechanicsDocument2 paginiMechanicsreynanÎncă nu există evaluări
- What Country Is Sushi FromDocument3 paginiWhat Country Is Sushi FromreynanÎncă nu există evaluări
- Ink ColorDocument4 paginiInk ColorreynanÎncă nu există evaluări
- Inclined Plane LabDocument2 paginiInclined Plane LabreynanÎncă nu există evaluări
- Excess Electrons Are Placed On A Small Lead Sphere With Mass So That Its Net Charge IsDocument1 paginăExcess Electrons Are Placed On A Small Lead Sphere With Mass So That Its Net Charge IsreynanÎncă nu există evaluări
- 1Document1 pagină1reynanÎncă nu există evaluări
- TOT Digestion of Food Science RevisedDocument4 paginiTOT Digestion of Food Science RevisedreynanÎncă nu există evaluări
- TITLE: Momentum PURPOSE: To Experimentally Find The Relationships Between Mass, Velocity, and Momentum. To Look at The LawDocument3 paginiTITLE: Momentum PURPOSE: To Experimentally Find The Relationships Between Mass, Velocity, and Momentum. To Look at The LawreynanÎncă nu există evaluări
- Central TendencyDocument105 paginiCentral TendencyreynanÎncă nu există evaluări
- FrictionDocument5 paginiFrictionreynanÎncă nu există evaluări
- Invalidate Your Answer.: Name: SectionDocument5 paginiInvalidate Your Answer.: Name: SectionreynanÎncă nu există evaluări
- IndustryDocument24 paginiIndustryreynanÎncă nu există evaluări
- ChemDocument15 paginiChemreynanÎncă nu există evaluări
- Charged spheres force net fields square charges accelerationDocument1 paginăCharged spheres force net fields square charges accelerationreynanÎncă nu există evaluări
- Solve For The Resultant Vector R 6. A 10m, 30° N of E 7. B 5m, 80° N of W 8. C 15m, SDocument1 paginăSolve For The Resultant Vector R 6. A 10m, 30° N of E 7. B 5m, 80° N of W 8. C 15m, SreynanÎncă nu există evaluări
- POKEMONDocument38 paginiPOKEMONMarco CuevasÎncă nu există evaluări
- Как устоновитьDocument1 paginăКак устоновитьKishore MaliÎncă nu există evaluări
- A Thermodynamic SystemDocument1 paginăA Thermodynamic SystemreynanÎncă nu există evaluări
- Big BangDocument93 paginiBig BangreynanÎncă nu există evaluări
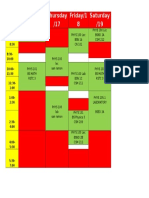
- Time Wednesda Y/16 Thursday /17 Friday/1 8 Saturday /19Document1 paginăTime Wednesda Y/16 Thursday /17 Friday/1 8 Saturday /19reynanÎncă nu există evaluări
- ChemDocument15 paginiChemreynanÎncă nu există evaluări
- QuizDocument2 paginiQuizreynanÎncă nu există evaluări
- MCQs in Strength of Materials Part I - Answers - PinoyBIXDocument5 paginiMCQs in Strength of Materials Part I - Answers - PinoyBIXreynanÎncă nu există evaluări
- 01 Intro To AstDocument134 pagini01 Intro To AstreynanÎncă nu există evaluări
- Big BangDocument93 paginiBig BangreynanÎncă nu există evaluări
- Jin 2001Document5 paginiJin 2001reynanÎncă nu există evaluări
- 2014 Fulbright Classic AppsDocument9 pagini2014 Fulbright Classic AppsChris RiveroÎncă nu există evaluări
- The Lumata Group - Hyperpolarized Magnetic Resonance LabDocument5 paginiThe Lumata Group - Hyperpolarized Magnetic Resonance LabreynanÎncă nu există evaluări
- Static FrictionDocument4 paginiStatic FrictionreynanÎncă nu există evaluări
- Illustrative Bank Branch Audit FormatDocument4 paginiIllustrative Bank Branch Audit Formatnil sheÎncă nu există evaluări
- Module 6 ObliCon Form Reformation and Interpretation of ContractsDocument6 paginiModule 6 ObliCon Form Reformation and Interpretation of ContractsAngelica BesinioÎncă nu există evaluări
- Understanding Cultural Awareness Ebook PDFDocument63 paginiUnderstanding Cultural Awareness Ebook PDFLaros Yudha100% (1)
- CH08 Location StrategyDocument45 paginiCH08 Location StrategyfatinS100% (5)
- Buku Drawing - REV - 02Document40 paginiBuku Drawing - REV - 02agung kurniawanÎncă nu există evaluări
- Stores & Purchase SopDocument130 paginiStores & Purchase SopRoshni Nathan100% (4)
- Đa S A The PESTEL Analysis of VinamilkDocument2 paginiĐa S A The PESTEL Analysis of VinamilkHiền ThảoÎncă nu există evaluări
- Business Math Notes PDFDocument12 paginiBusiness Math Notes PDFCzareena Sulica DiamaÎncă nu există evaluări
- AZ 104 - Exam Topics Testlet 07182023Document28 paginiAZ 104 - Exam Topics Testlet 07182023vincent_phlÎncă nu există evaluări
- PDEA Joint AffidavitDocument1 paginăPDEA Joint Affidavitlevis sy100% (1)
- Your Guide To Starting A Small EnterpriseDocument248 paginiYour Guide To Starting A Small Enterprisekleomarlo94% (18)
- Skills 360 - Negotiations 2: Making The Deal: Discussion QuestionsDocument6 paginiSkills 360 - Negotiations 2: Making The Deal: Discussion QuestionsTrần ThơmÎncă nu există evaluări
- Tawfīq Al - Akīm and The West PDFDocument12 paginiTawfīq Al - Akīm and The West PDFCosmin MaricaÎncă nu există evaluări
- Evolution of Local Bodies in IndiaDocument54 paginiEvolution of Local Bodies in Indiaanashwara.pillaiÎncă nu există evaluări
- Schedule of Rates for LGED ProjectsDocument858 paginiSchedule of Rates for LGED ProjectsRahul Sarker40% (5)
- International Conference GREDIT 2016Document1 paginăInternational Conference GREDIT 2016Οδυσσεας ΚοψιδαςÎncă nu există evaluări
- Advocacy PresentationDocument13 paginiAdvocacy Presentationapi-459424184Încă nu există evaluări
- Jffii - Google SearchDocument2 paginiJffii - Google SearchHAMMAD SHAHÎncă nu există evaluări
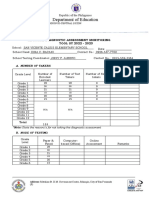
- Regional Diagnostic Assessment Report SY 2022-2023Document3 paginiRegional Diagnostic Assessment Report SY 2022-2023Dina BacaniÎncă nu există evaluări
- Kanter v. BarrDocument64 paginiKanter v. BarrTodd Feurer100% (1)
- Exercise of Caution: Read The Text To Answer Questions 3 and 4Document3 paginiExercise of Caution: Read The Text To Answer Questions 3 and 4Shantie Susan WijayaÎncă nu există evaluări
- Elementary Present Continuous and Present Simple AnswersDocument5 paginiElementary Present Continuous and Present Simple AnswersFabio SoaresÎncă nu există evaluări
- Selected Candidates For The Post of Stenotypist (BS-14), Open Merit QuotaDocument6 paginiSelected Candidates For The Post of Stenotypist (BS-14), Open Merit Quotaامین ثانیÎncă nu există evaluări
- English Final Suggestion - HSC - 2013Document8 paginiEnglish Final Suggestion - HSC - 2013Jaman Palash (MSP)Încă nu există evaluări
- Factors Affecting Exclusive BreastfeedingDocument7 paginiFactors Affecting Exclusive BreastfeedingPuput Dwi PuspitasariÎncă nu există evaluări
- Introduction To World Religion and Belief Systems: Ms. Niña A. Sampaga Subject TeacherDocument65 paginiIntroduction To World Religion and Belief Systems: Ms. Niña A. Sampaga Subject Teacherniña sampagaÎncă nu există evaluări
- Tata Securities BranchesDocument6 paginiTata Securities BranchesrakeyyshÎncă nu există evaluări
- Class: 3 LPH First Term English Test Part One: Reading: A/ Comprehension (07 PTS)Document8 paginiClass: 3 LPH First Term English Test Part One: Reading: A/ Comprehension (07 PTS)DjihedÎncă nu există evaluări
- IMMI Refusal Notification With Decision Record-4Document6 paginiIMMI Refusal Notification With Decision Record-4SHREYAS JOSHIÎncă nu există evaluări
- The Great MughalsDocument14 paginiThe Great MughalsnikitaÎncă nu există evaluări