S-ar putea să vă placă și
- Management and Administration Skills for the Mental Health ProfessionalDe la EverandManagement and Administration Skills for the Mental Health ProfessionalÎncă nu există evaluări
- Treatment Modalities Applicable To The Psychiatric ClientDocument53 paginiTreatment Modalities Applicable To The Psychiatric Clientnickybore100% (1)
- Elmeida Effendy Department of Psychiatry Medical Faculty-USUDocument31 paginiElmeida Effendy Department of Psychiatry Medical Faculty-USUYolanda SimamoraÎncă nu există evaluări
- Disability Behaviour Support Skill Set Facilitator GuideDocument43 paginiDisability Behaviour Support Skill Set Facilitator GuideMirela Cojocaru StetcoÎncă nu există evaluări
- Handling Difficult Patient BehaviorsDocument4 paginiHandling Difficult Patient BehaviorsneuronurseÎncă nu există evaluări
- Mental Health GuidanceDocument93 paginiMental Health GuidanceRamona Iocsa PoraÎncă nu există evaluări
- Implementing Human Factors in Healthcare: A 'How to' GuideDocument34 paginiImplementing Human Factors in Healthcare: A 'How to' GuideChiwong KoerÎncă nu există evaluări
- Mental Health of Older Adults: Facts, Risks & WHO ResponseDocument6 paginiMental Health of Older Adults: Facts, Risks & WHO Responsesergius3Încă nu există evaluări
- Stress Management Policy ProcedureDocument4 paginiStress Management Policy ProcedurelkulahÎncă nu există evaluări
- 2015 Final Case Studies Asam Fundamentals Final UpdatedDocument68 pagini2015 Final Case Studies Asam Fundamentals Final UpdatedTrampa AdelinaÎncă nu există evaluări
- Psychological ChangesDocument36 paginiPsychological ChangesAndrei La MadridÎncă nu există evaluări
- DRAFT Mental Wellbeing Policy 2016Document3 paginiDRAFT Mental Wellbeing Policy 2016Candice HurstÎncă nu există evaluări
- Anti Social Personality HandoutDocument4 paginiAnti Social Personality HandoutErfana ThasnemÎncă nu există evaluări
- Psychiatric and Mental Health NursingDocument10 paginiPsychiatric and Mental Health NursingGlaiza Claire Am-amlan OlayanÎncă nu există evaluări
- Comorbidity Guideline PDFDocument446 paginiComorbidity Guideline PDFglenÎncă nu există evaluări
- IASC Guidelines Mental Health Psycho Social SupportDocument99 paginiIASC Guidelines Mental Health Psycho Social SupportCristina Bucataru100% (1)
- Chapter 23 Disruptive Beahvior DisordersDocument5 paginiChapter 23 Disruptive Beahvior DisordersCatia FernandesÎncă nu există evaluări
- Understanding Dementia Through a Case StudyDocument42 paginiUnderstanding Dementia Through a Case StudyJay VillasotoÎncă nu există evaluări
- Managing The Aggressive and Violent Patient in The Psychiatric EmergencyDocument13 paginiManaging The Aggressive and Violent Patient in The Psychiatric Emergencyana100% (1)
- Attitudes Toward Sex and Relationships. The Second Australian Study of Health and RelationshipsDocument9 paginiAttitudes Toward Sex and Relationships. The Second Australian Study of Health and Relationshipsfelipegonzalezfg1Încă nu există evaluări
- The Art of Social Prescribing - Kerry WilsonDocument14 paginiThe Art of Social Prescribing - Kerry WilsonNCVOÎncă nu există evaluări
- Standards of Psychiatric NursingDocument19 paginiStandards of Psychiatric Nursingamita chaudhari50% (2)
- Medical Social WorkDocument28 paginiMedical Social WorkKirubakaran Harry67% (3)
- Mental Status EvaluationDocument7 paginiMental Status Evaluationmunir houseÎncă nu există evaluări
- 3 - Mood DisordersDocument44 pagini3 - Mood DisordersBoss --Încă nu există evaluări
- Substance - Related Addictive DisordersDocument43 paginiSubstance - Related Addictive DisordersMarinel June PalerÎncă nu există evaluări
- NDIS Operational Procedures FBI 2005Document32 paginiNDIS Operational Procedures FBI 2005jac_blakeÎncă nu există evaluări
- Screening Tools For PostpartumDocument9 paginiScreening Tools For PostpartumNeni RochmayatiÎncă nu există evaluări
- Code of Ethics 2017 Edition Secure Interactive PDFDocument60 paginiCode of Ethics 2017 Edition Secure Interactive PDFJade BouchardÎncă nu există evaluări
- Psychiatry Operational Policy PDFDocument124 paginiPsychiatry Operational Policy PDFZaida NorÎncă nu există evaluări
- Therapeutic Communication in Psychiatric NursingDocument7 paginiTherapeutic Communication in Psychiatric NursingKatrina BuenconsejoÎncă nu există evaluări
- Psychiatric AssignmentDocument2 paginiPsychiatric AssignmentArlene Macatangay100% (1)
- Abuse and Violence: Abuse Is The Wrongful Use and Maltreatment of Another PersonDocument10 paginiAbuse and Violence: Abuse Is The Wrongful Use and Maltreatment of Another PersonjacnpoyÎncă nu există evaluări
- MENTAL HEALTH NURSING STANDARDSDocument33 paginiMENTAL HEALTH NURSING STANDARDSSANU RAMASWAMY100% (1)
- Guidance on Risk Management in Mental HealthDocument54 paginiGuidance on Risk Management in Mental Healthjazz8181Încă nu există evaluări
- 80198ef2d8bc6630f85fd88314a2a8d6risk_governance_and_patient_safetyDocument16 pagini80198ef2d8bc6630f85fd88314a2a8d6risk_governance_and_patient_safetyadityaukavalaÎncă nu există evaluări
- Short Answers of Week 6: Assessment 1Document8 paginiShort Answers of Week 6: Assessment 1Rija Syeda HaqueÎncă nu există evaluări
- Osborne+et+al +the+health+education+impact+questionnaireDocument10 paginiOsborne+et+al +the+health+education+impact+questionnairesandrine.abellarÎncă nu există evaluări
- Kuwait Declaration On Patient SafetyDocument5 paginiKuwait Declaration On Patient Safetyanita astaliaÎncă nu există evaluări
- Who Uhl Ihs PSF 2022.3 EngDocument5 paginiWho Uhl Ihs PSF 2022.3 Engmellysawitri9Încă nu există evaluări
- Risk Governance and patient safetyDocument26 paginiRisk Governance and patient safetyadityaukavalaÎncă nu există evaluări
- Nurses' Adherence To Patient Safety Principles: A Systematic ReviewDocument15 paginiNurses' Adherence To Patient Safety Principles: A Systematic ReviewWidia Hertina PutriÎncă nu există evaluări
- Patient Safety Strategy 2022Document13 paginiPatient Safety Strategy 2022Megersa AleneÎncă nu există evaluări
- Risk Management StrategyDocument37 paginiRisk Management StrategyanhvufÎncă nu există evaluări
- Quality Assurance and Patient Safety Measures: A Comparative Longitudinal AnalysisDocument8 paginiQuality Assurance and Patient Safety Measures: A Comparative Longitudinal AnalysisjyothiÎncă nu există evaluări
- 41 06 Integrated Risk Management FrameworkDocument22 pagini41 06 Integrated Risk Management FrameworksarifinÎncă nu există evaluări
- Rapid Risk Assessment of Acute Public Health EventsDocument44 paginiRapid Risk Assessment of Acute Public Health EventsdinahajjarÎncă nu există evaluări
- Risk Management Policy - NHSDocument32 paginiRisk Management Policy - NHSDewi Ratna Sari100% (1)
- Risk Register & Assessment GuideDocument24 paginiRisk Register & Assessment GuideAgus Dohardo ManaluÎncă nu există evaluări
- Patient Safety Initiative Hospital Executive and Physician Leadership StrategiesDocument39 paginiPatient Safety Initiative Hospital Executive and Physician Leadership StrategiesDian Kharisma100% (1)
- About Us: Patient SafetyDocument7 paginiAbout Us: Patient SafetyFaulya Nurmala ArovaÎncă nu există evaluări
- Clinical GovernanceDocument66 paginiClinical Governanceummuawisy100% (2)
- Infection Control NHS PolicyDocument12 paginiInfection Control NHS PolicyYahya Salem100% (1)
- Analysis of A Healthcare Risk Management PlanDocument6 paginiAnalysis of A Healthcare Risk Management PlanGeralds B GeraldÎncă nu există evaluări
- Flinders Program Information PaperDocument9 paginiFlinders Program Information PaperIbheenk WMÎncă nu există evaluări
- 2 Pasos Seguridad PteDocument12 pagini2 Pasos Seguridad PteLUCAS coronelÎncă nu există evaluări
- Clinical Risk ManagementDocument3 paginiClinical Risk Managementshivam1969Încă nu există evaluări
- Scope of Practice For RN DHA PDFDocument18 paginiScope of Practice For RN DHA PDFRrichard Prieto MmallariÎncă nu există evaluări
- Implementation of A Sustainable Enterprise Risk Management Framework: The Administrator On Duty ModelDocument8 paginiImplementation of A Sustainable Enterprise Risk Management Framework: The Administrator On Duty ModelRudi UtomoÎncă nu există evaluări
- 2018 - 22nd Brochure PagesDocument6 pagini2018 - 22nd Brochure Pagesyos_peace86Încă nu există evaluări
- Leadership Styles and Employee Motivation in Qatar OrganizationsDocument14 paginiLeadership Styles and Employee Motivation in Qatar Organizationsyos_peace86Încă nu există evaluări
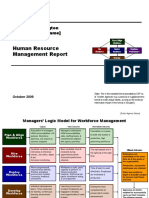
- Human Resource Management Report: State of Washington (Enter Agency Name)Document19 paginiHuman Resource Management Report: State of Washington (Enter Agency Name)Bounna PhoumalavongÎncă nu există evaluări
- 2019 Research Symposium RulesDocument10 pagini2019 Research Symposium Rulesyos_peace86Încă nu există evaluări
- People Strategy Summary SlidesDocument15 paginiPeople Strategy Summary SlidesAbdullah Kilawi50% (2)
- 3Rd Annual Transformational Ophthalmology Symposium: Saturday, OCTOBER 6, 2018 8:00 AM - 4:00 PMDocument5 pagini3Rd Annual Transformational Ophthalmology Symposium: Saturday, OCTOBER 6, 2018 8:00 AM - 4:00 PMyos_peace86Încă nu există evaluări
- Booklet Simpozium en Web-1Document6 paginiBooklet Simpozium en Web-1yos_peace86Încă nu există evaluări
- Leadership Styles and Employee Motivation in Qatar Organizations PDFDocument148 paginiLeadership Styles and Employee Motivation in Qatar Organizations PDFyos_peace86Încă nu există evaluări
- IPOSFlyer2018!4!11 WebDocument2 paginiIPOSFlyer2018!4!11 Webyos_peace86Încă nu există evaluări
- 2018 Neuroscience Symposium: Friday, April 27, 2018 7:30 A.M. To 4:30 P.MDocument6 pagini2018 Neuroscience Symposium: Friday, April 27, 2018 7:30 A.M. To 4:30 P.Myos_peace86Încă nu există evaluări
- Revised Conference at A Glance 13Document2 paginiRevised Conference at A Glance 13yos_peace86Încă nu există evaluări
- Stroke & Neurological Disease Conference: Ninth AnnualDocument2 paginiStroke & Neurological Disease Conference: Ninth Annualyos_peace86Încă nu există evaluări
- Western New York Neuroscience Symposium: (Paddock Room)Document2 paginiWestern New York Neuroscience Symposium: (Paddock Room)yos_peace86Încă nu există evaluări
- NEU 15-746 BroDocument2 paginiNEU 15-746 Broyos_peace86Încă nu există evaluări
- 2018 Child Neurology Flyer v6Document1 pagină2018 Child Neurology Flyer v6yos_peace86Încă nu există evaluări
- Paeds Flyer and Application Form 2018Document2 paginiPaeds Flyer and Application Form 2018yos_peace86Încă nu există evaluări
- Neurorheum Conf May 2015Document4 paginiNeurorheum Conf May 2015yos_peace86Încă nu există evaluări
- 27013Document12 pagini27013yos_peace86Încă nu există evaluări
- Patient BrochureDocument3 paginiPatient Brochureyos_peace86Încă nu există evaluări
- Conference/Symposium Evaluation Form: 1 Poor 2 Below Average 3 Average 4 Above Average 5 OutstandingDocument2 paginiConference/Symposium Evaluation Form: 1 Poor 2 Below Average 3 Average 4 Above Average 5 Outstandingyos_peace86Încă nu există evaluări
- Sponsorship Document - Symposium 2018Document4 paginiSponsorship Document - Symposium 2018yos_peace86Încă nu există evaluări
- DENT Neurologic CME 2018 ProgramDocument4 paginiDENT Neurologic CME 2018 Programyos_peace86Încă nu există evaluări
- Sports Dentistry Symposium RegistrationDocument1 paginăSports Dentistry Symposium Registrationyos_peace86Încă nu există evaluări
- Tri-Society Restorative Symposium 2018Document9 paginiTri-Society Restorative Symposium 2018yos_peace86Încă nu există evaluări
- Virginia Liver Symposium & Update in Gastroenterology: The 22nd AnnualDocument4 paginiVirginia Liver Symposium & Update in Gastroenterology: The 22nd Annualyos_peace86Încă nu există evaluări
- Brochure Temple OrthoSymposium2018 ADocument5 paginiBrochure Temple OrthoSymposium2018 Ayos_peace86Încă nu există evaluări
- Isdh 2019 Sponsorship ProspectusDocument12 paginiIsdh 2019 Sponsorship Prospectusyos_peace86Încă nu există evaluări
- Survival Skills Page by PageDocument6 paginiSurvival Skills Page by Pageyos_peace86Încă nu există evaluări
- Patient BrochureDocument3 paginiPatient Brochureyos_peace86Încă nu există evaluări
- 2017 Stroke SymposiumDocument6 pagini2017 Stroke Symposiumyos_peace86Încă nu există evaluări
- The Happiness EffectDocument2 paginiThe Happiness EffectClaudene GellaÎncă nu există evaluări
- Breaking The Silence: The Hidden Injuries of Neo-Liberal AcademiaDocument21 paginiBreaking The Silence: The Hidden Injuries of Neo-Liberal AcademiaGiulia PalladiniÎncă nu există evaluări
- Understanding the Functions of ArtDocument5 paginiUnderstanding the Functions of ArtJayArt Amogis TemPoralÎncă nu există evaluări
- Adjudication Considerations For British Parliamentary Debate PDFDocument20 paginiAdjudication Considerations For British Parliamentary Debate PDFAcbel Rnuco100% (1)
- BSP Phase1 Manual David Grand 2Document117 paginiBSP Phase1 Manual David Grand 2Muhamad LuthfillahÎncă nu există evaluări
- Thematic Guide To Young Adult LiteratureDocument269 paginiThematic Guide To Young Adult LiteratureJ S ShineÎncă nu există evaluări
- Plan de LectieDocument4 paginiPlan de LectieIonelaDnyÎncă nu există evaluări
- Intelligence PDFDocument19 paginiIntelligence PDFmiji_ggÎncă nu există evaluări
- Sentence WritingDocument2 paginiSentence WritingLee Mei Chai李美齊Încă nu există evaluări
- The Arts in Psychotherapy: Suzanne Haeyen, Lisa HinzDocument6 paginiThe Arts in Psychotherapy: Suzanne Haeyen, Lisa HinzSn. DharmajyotiÎncă nu există evaluări
- Bridges FOR Communication AND Information: Reyjen C. PresnoDocument27 paginiBridges FOR Communication AND Information: Reyjen C. PresnoReyjen PresnoÎncă nu există evaluări
- Management Principles for Guiding DecisionsDocument3 paginiManagement Principles for Guiding DecisionsKamal Kamalmba100% (1)
- EAP Grammar-Decomposing Long Complex SentencesDocument2 paginiEAP Grammar-Decomposing Long Complex SentencesKevinchcÎncă nu există evaluări
- W Astin Implement The Strategies and Rubric - Module 4Document6 paginiW Astin Implement The Strategies and Rubric - Module 4api-325932544Încă nu există evaluări
- Play TherapyDocument26 paginiPlay TherapypastellarÎncă nu există evaluări
- Group Synergy in Problem SolvingDocument29 paginiGroup Synergy in Problem SolvingKenny Ann Grace BatiancilaÎncă nu există evaluări
- Secondary school classes in DrariaDocument2 paginiSecondary school classes in DrariaMrm ZwlyÎncă nu există evaluări
- If How Tos Were EnoughDocument57 paginiIf How Tos Were Enoughapi-3745547Încă nu există evaluări
- Eugenia Kaw - Opening Faces - The Politics of Cosmetic Surgery and Asian American Women PDFDocument20 paginiEugenia Kaw - Opening Faces - The Politics of Cosmetic Surgery and Asian American Women PDFAllison HsuÎncă nu există evaluări
- Rubric For Ad Project - Part 3 - PitchDocument1 paginăRubric For Ad Project - Part 3 - Pitchapi-231413786100% (1)
- 01797johari WindowDocument23 pagini01797johari WindowAjay Kumar ChoudharyÎncă nu există evaluări
- A Study of Effectiveness of A Programme Developed To Improve The Marathi Pronunciation of 4 STD English Medium StudentsDocument32 paginiA Study of Effectiveness of A Programme Developed To Improve The Marathi Pronunciation of 4 STD English Medium StudentsSOHEL BANGIÎncă nu există evaluări
- Qualitative Data AnalysisDocument4 paginiQualitative Data AnalysisShambhav Lama100% (1)
- Chapter 3 Authority Power InfluenceDocument18 paginiChapter 3 Authority Power InfluenceChaps Bryan Catama100% (2)
- Safety Incentive ProgramDocument18 paginiSafety Incentive ProgramasokÎncă nu există evaluări
- Understanding Conflict Resolutio - Hilal AhmadDocument8 paginiUnderstanding Conflict Resolutio - Hilal Ahmadjaseme7579Încă nu există evaluări
- Mental Stress Evaluation Using Heart Rate Variability AnalysisDocument7 paginiMental Stress Evaluation Using Heart Rate Variability AnalysisKalpeshPatilÎncă nu există evaluări
- Chapter 4 About Mental HealthDocument6 paginiChapter 4 About Mental HealthPinsanity GoalsÎncă nu există evaluări
- 1 - Looking at Language Learning StrategiesDocument18 pagini1 - Looking at Language Learning StrategiesTami MolinaÎncă nu există evaluări
- Unit Plan-Badminton Jenna Maceachen: Subject Area Grade Level Topic Length of Unit (Days)Document8 paginiUnit Plan-Badminton Jenna Maceachen: Subject Area Grade Level Topic Length of Unit (Days)api-507324305Încă nu există evaluări