S-ar putea să vă placă și
- Disease Detectives NotesDocument5 paginiDisease Detectives NotesErica Weng0% (1)
- Hiv Treatment: IC2 Haemato-Lymphoid and Tropical Medicine HLTM Dr. Eoghan de Barra 2014Document55 paginiHiv Treatment: IC2 Haemato-Lymphoid and Tropical Medicine HLTM Dr. Eoghan de Barra 2014Faiq Syukri Bin SaparudinÎncă nu există evaluări
- The Ear and It's DisordersDocument104 paginiThe Ear and It's DisordersAyaBasilioÎncă nu există evaluări
- Ryan Martin Ko, M.DDocument54 paginiRyan Martin Ko, M.DDhaval Makwana100% (2)
- Vestibular Disorder Guide (updated 09/06Document6 paginiVestibular Disorder Guide (updated 09/06Ecaterina ChiriacÎncă nu există evaluări
- Opthhalmology Examination ReviewDocument12 paginiOpthhalmology Examination ReviewFaiq Syukri Bin SaparudinÎncă nu există evaluări
- The EarDocument59 paginiThe EarJasmin Jacob100% (5)
- Ears, Nose and Throat Diseases: Prepared By: Hannelli BelingonDocument103 paginiEars, Nose and Throat Diseases: Prepared By: Hannelli BelingonPatricia Kamille I. PawidÎncă nu există evaluări
- Mineire'sDocument16 paginiMineire'sShaykh Evangelista BacualÎncă nu există evaluări
- How To Perform Clinical AuditDocument70 paginiHow To Perform Clinical AuditFaiq Syukri Bin SaparudinÎncă nu există evaluări
- Ent and OptalmologyDocument138 paginiEnt and OptalmologyFan Eli100% (3)
- Vet MedicinesDocument36 paginiVet MedicinesSadam Irshad100% (3)
- Assessment and Management of Patients With Hearing and Balance Disorders WebDocument36 paginiAssessment and Management of Patients With Hearing and Balance Disorders WebStephKirstin Velasco Malapit100% (2)
- Hearing LossDocument31 paginiHearing LossDat boi100% (1)
- HEARING LOSS GUIDEDocument46 paginiHEARING LOSS GUIDEgibreilÎncă nu există evaluări
- Musculoskeletal Imaging 2015Document79 paginiMusculoskeletal Imaging 2015Faiq Syukri Bin SaparudinÎncă nu există evaluări
- Diseases of Pulp and PeriapicalDocument70 paginiDiseases of Pulp and PeriapicalAkash Anilkumar MaliniÎncă nu există evaluări
- EarDocument33 paginiEarHikmat UllahÎncă nu există evaluări
- Medical Epidemiology MCQDocument12 paginiMedical Epidemiology MCQFaiq Syukri Bin Saparudin82% (165)
- Introduction To Pediatric Radiology Pediatric Radiology Online Course by Dr. Ashraf Abotaleb PDFDocument436 paginiIntroduction To Pediatric Radiology Pediatric Radiology Online Course by Dr. Ashraf Abotaleb PDFRicardo VallejoÎncă nu există evaluări
- Ent Case 2Document29 paginiEnt Case 2Trina CardonaÎncă nu există evaluări
- Contrast Media in Diagnostic RadiologyDocument56 paginiContrast Media in Diagnostic RadiologyFaiq Syukri Bin SaparudinÎncă nu există evaluări
- Seminar On Infetion ControlDocument76 paginiSeminar On Infetion ControlDaisy Vinu0% (1)
- Hearing Loss (Deafness), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandHearing Loss (Deafness), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsEvaluare: 4 din 5 stele4/5 (1)
- Pseudomonas BasicsDocument32 paginiPseudomonas Basicstummalapalli venkateswara raoÎncă nu există evaluări
- Oral Rehabilitation With Removable Partial Dentures in Advanced Tooth Loss SituationsDocument7 paginiOral Rehabilitation With Removable Partial Dentures in Advanced Tooth Loss SituationsIoana-NicoletaNicodimÎncă nu există evaluări
- PRACTICE TEACHING On Otitis Media FinalDocument33 paginiPRACTICE TEACHING On Otitis Media FinalAjit ThangeÎncă nu există evaluări
- 2012 ENT OSCE QuestionsDocument4 pagini2012 ENT OSCE QuestionsFaiq Syukri Bin Saparudin50% (2)
- Assessment of The Ear, Nose and ThroatDocument40 paginiAssessment of The Ear, Nose and Throatsnickers_j100% (3)
- Managing ENT DisordersDocument26 paginiManaging ENT DisordersShreyas Walvekar100% (3)
- Assessing The Ears and HearingDocument22 paginiAssessing The Ears and HearingGrace RamosÎncă nu există evaluări
- Understanding Otitis Media: Causes, Symptoms and Treatment of Ear InfectionsDocument98 paginiUnderstanding Otitis Media: Causes, Symptoms and Treatment of Ear InfectionsLody Lean CruzÎncă nu există evaluări
- The EarDocument1 paginăThe EarAnonymous 8KN8IR1GTWÎncă nu există evaluări
- Eye and Ear DisordersDocument14 paginiEye and Ear Disorderslemesa abdisaÎncă nu există evaluări
- Acuite Otitis Media Final PresentationDocument26 paginiAcuite Otitis Media Final Presentationmohamedkallon1996Încă nu există evaluări
- Ear Pathology GuideDocument34 paginiEar Pathology Guidenagham hamdanÎncă nu există evaluări
- Conductive Hearing Loss (Tuli Konduktif)Document29 paginiConductive Hearing Loss (Tuli Konduktif)Sena AjahÎncă nu există evaluări
- ENT - UnitDocument63 paginiENT - Unitsuganthi rajesh kannaÎncă nu există evaluări
- Krishna Reddy OTALGIA AND TINNITUS FinalDocument14 paginiKrishna Reddy OTALGIA AND TINNITUS FinalSiva ramaÎncă nu există evaluări
- Drugs and Substance AbuseDocument75 paginiDrugs and Substance Abuseseline sherylÎncă nu există evaluări
- Anatomy of the Ear: External, Middle, Inner Structures and Common Conditions (39Document55 paginiAnatomy of the Ear: External, Middle, Inner Structures and Common Conditions (39Hershey Cordero BrionesÎncă nu există evaluări
- ENT Lectures 1Document123 paginiENT Lectures 1lxnalexander100% (1)
- Ha - Asssessing EarsDocument6 paginiHa - Asssessing EarsKenneth Andre Batuyog TecsonÎncă nu există evaluări
- Hearing Loss Assessment and Treatment GuideDocument31 paginiHearing Loss Assessment and Treatment GuideKIBET ERNEST MUTAIÎncă nu există evaluări
- Ear - Islam AssiDocument21 paginiEar - Islam AssiIslam AssiÎncă nu există evaluări
- Ear ChronicDocument44 paginiEar ChronicȜLaa AsHrafÎncă nu există evaluări
- Chapter 15 Disorders of The Eyes and EarsDocument42 paginiChapter 15 Disorders of The Eyes and Earskelsey jacksonÎncă nu există evaluări
- Symptom A To Logy of EarDocument36 paginiSymptom A To Logy of Ear98480sam23006100% (1)
- Otitis MediaDocument55 paginiOtitis MediaJollyann SedaÎncă nu există evaluări
- A. Nasal Symptoms 1. Nasal Obstruction Is The Commonest Symptom. - This Leads To MouthDocument6 paginiA. Nasal Symptoms 1. Nasal Obstruction Is The Commonest Symptom. - This Leads To MouthRubi MeeajanÎncă nu există evaluări
- CASE ANALYSIS - Chronic TympanomastoiditisDocument5 paginiCASE ANALYSIS - Chronic TympanomastoiditisTerry Mae Atilazal SarciaÎncă nu există evaluări
- Presentations of Middle Ear Disease: Elizabeth Rose Royal Victorian Eye and Ear Hospital Royal Children's HospitalDocument43 paginiPresentations of Middle Ear Disease: Elizabeth Rose Royal Victorian Eye and Ear Hospital Royal Children's Hospitalathe_triiaÎncă nu există evaluări
- 7 - Ear 1Document40 pagini7 - Ear 1Touseeq ManzoorÎncă nu există evaluări
- Assessment and Management of Patients With Hearing and Balance DisordersDocument9 paginiAssessment and Management of Patients With Hearing and Balance Disordersxhemhae100% (1)
- THT: IntroducingDocument33 paginiTHT: IntroducingqurataÎncă nu există evaluări
- مراجعة الأوسكىDocument238 paginiمراجعة الأوسكىHala BahaaÎncă nu există evaluări
- Pathophysiology and Complications of CSOM ExplainedDocument42 paginiPathophysiology and Complications of CSOM ExplainedSalsabilla Ameranti PutriÎncă nu există evaluări
- Second DayDocument47 paginiSecond DayMeryville JacildoÎncă nu există evaluări
- Otitis MediaDocument6 paginiOtitis MediaAbdullah EssaÎncă nu există evaluări
- What Is The EarDocument5 paginiWhat Is The EarernalifehouseÎncă nu există evaluări
- Ear BulletsDocument3 paginiEar BulletsDonaJeanÎncă nu există evaluări
- Chronic Suppurative Otitis Media (CSOM)Document31 paginiChronic Suppurative Otitis Media (CSOM)Mimo HemadÎncă nu există evaluări
- Chronic Otitis Media (Mesotympanitis. Epitympanitis) - Otogenous Intracranial ComplicationsDocument53 paginiChronic Otitis Media (Mesotympanitis. Epitympanitis) - Otogenous Intracranial Complicationssimi yÎncă nu există evaluări
- O To SclerosisDocument44 paginiO To Sclerosismajhi.jhalak19Încă nu există evaluări
- Osteoma of Facial Nerve Canal With Cholesteatoma: A Rarest of Rare PresentationDocument5 paginiOsteoma of Facial Nerve Canal With Cholesteatoma: A Rarest of Rare PresentationalvaputriÎncă nu există evaluări
- Anatomy of Human EarDocument5 paginiAnatomy of Human EarSharanz Twentyfour SevenÎncă nu există evaluări
- Otits MediaDocument68 paginiOtits MediaSaidi EdwardÎncă nu există evaluări
- 2-E. N. T. 2Document3 pagini2-E. N. T. 2Ema FröhlichováÎncă nu există evaluări
- Ear Disorders: Causes, Symptoms and TreatmentsDocument65 paginiEar Disorders: Causes, Symptoms and TreatmentsMonica JubaneÎncă nu există evaluări
- Common ENT Conditions PresentationDocument60 paginiCommon ENT Conditions PresentationMICHAEL SAKALAÎncă nu există evaluări
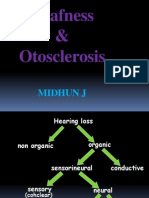
- Deafness & Otosclerosis: Midhun JDocument44 paginiDeafness & Otosclerosis: Midhun JRohit R PillaiÎncă nu există evaluări
- Presentation Otitis ExternaDocument24 paginiPresentation Otitis ExternaRichard GunawanÎncă nu există evaluări
- Menieres DiseaseDocument40 paginiMenieres DiseaseXenia Marie Razalo LawanÎncă nu există evaluări
- ENT Conditions: Hearing Loss, Balance Issues, Tinnitus & MoreDocument24 paginiENT Conditions: Hearing Loss, Balance Issues, Tinnitus & MoreBalakrishnan DoraisamiÎncă nu există evaluări
- Paediatric History 2013Document3 paginiPaediatric History 2013Faiq Syukri Bin SaparudinÎncă nu există evaluări
- Osce Example DR Tbalu's EntDocument20 paginiOsce Example DR Tbalu's EntFaiq Syukri Bin SaparudinÎncă nu există evaluări
- Radiation HazardDocument40 paginiRadiation HazardFaiq Syukri Bin SaparudinÎncă nu există evaluări
- Age-Related Macular Degeneration - Ophthalmology - FastbleepDocument5 paginiAge-Related Macular Degeneration - Ophthalmology - FastbleepFaiq Syukri Bin SaparudinÎncă nu există evaluări
- Cataract - Ophthalmology - FastbleepDocument9 paginiCataract - Ophthalmology - FastbleepFaiq Syukri Bin SaparudinÎncă nu există evaluări
- Red Eye - Ophthalmology - FastbleepDocument6 paginiRed Eye - Ophthalmology - FastbleepFaiq Syukri Bin SaparudinÎncă nu există evaluări
- NS - 30 - Addiction - 2013 16oct PDFDocument53 paginiNS - 30 - Addiction - 2013 16oct PDFFaiq Syukri Bin SaparudinÎncă nu există evaluări
- HN1. Cervical - SpineDocument29 paginiHN1. Cervical - SpineFaiq Syukri Bin SaparudinÎncă nu există evaluări
- New Drug 2010 Upto Aug 2010Document15 paginiNew Drug 2010 Upto Aug 2010NAVNEET BAGGAÎncă nu există evaluări
- HUMAN HERPES VIRUS Types 6Document1 paginăHUMAN HERPES VIRUS Types 6api-3704562100% (1)
- Survey DesignDocument66 paginiSurvey DesignAbdul HadiÎncă nu există evaluări
- Influenza 1918.0910Document19 paginiInfluenza 1918.0910RafaelÎncă nu există evaluări
- 1st Long Test in HealthDocument1 pagină1st Long Test in HealthRovilyn Dizon71% (7)
- An Etiological Reappraisal of Pancytopenia - LargestDocument9 paginiAn Etiological Reappraisal of Pancytopenia - LargestKaye Antonette AntioquiaÎncă nu există evaluări
- Agustin, Aileen - CMV UL 16Document10 paginiAgustin, Aileen - CMV UL 16Concepcion R. AquinoÎncă nu există evaluări
- Ophthalmic Medical Intervention IDocument3 paginiOphthalmic Medical Intervention Igideon A. owusu0% (1)
- 5P MEDICINE2 Valvular Heart Disease 1 - Dr. Rene ManaloDocument6 pagini5P MEDICINE2 Valvular Heart Disease 1 - Dr. Rene Manalok.n.e.d.Încă nu există evaluări
- Microbiological Guidelines For Ready-To-Eat FoodsDocument5 paginiMicrobiological Guidelines For Ready-To-Eat Foodscaya1172Încă nu există evaluări
- ISR Project - Water Scarcity in MaharashtraDocument38 paginiISR Project - Water Scarcity in MaharashtraSuraj0% (2)
- KAP of child immunization in KalabaydhDocument61 paginiKAP of child immunization in Kalabaydhmona gamadid100% (2)
- Susan G Komen EssayDocument6 paginiSusan G Komen Essayapi-248182825Încă nu există evaluări
- Vulvar Ulcer CausesDocument4 paginiVulvar Ulcer CausesChibiÎncă nu există evaluări
- Miko SisDocument90 paginiMiko SisFahlevi QalbiÎncă nu există evaluări
- Diseases of The Pharynx: BY DR Arif Raza Khan Assistant Professor E.N.T. K.T.HDocument29 paginiDiseases of The Pharynx: BY DR Arif Raza Khan Assistant Professor E.N.T. K.T.HSuleman MuhammadÎncă nu există evaluări
- Cumle Doldurma TEST2 PDFDocument6 paginiCumle Doldurma TEST2 PDFmetinÎncă nu există evaluări
- Estimating the True Prevalence of Fasciola hepatica in Swiss CattleDocument6 paginiEstimating the True Prevalence of Fasciola hepatica in Swiss CattleMuhammad FaridÎncă nu există evaluări
- CDC E. Coli FactsheetDocument2 paginiCDC E. Coli Factsheetbutter-mmÎncă nu există evaluări
- Cilium: Cell Organelle with Sensory and Motility FunctionsDocument5 paginiCilium: Cell Organelle with Sensory and Motility FunctionsMuhammad ZairulfikriÎncă nu există evaluări
- Epidemiologi of HFMDDocument16 paginiEpidemiologi of HFMDJimmy AmbaritaÎncă nu există evaluări
- Prolonged and Postterm Pregnancy: Roxane Rampersad and George A. MaconesDocument7 paginiProlonged and Postterm Pregnancy: Roxane Rampersad and George A. MaconesAphreLbecasean WaeÎncă nu există evaluări