S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- National CPR Association ACLS Study GuideDocument18 paginiNational CPR Association ACLS Study Guidekumar23Încă nu există evaluări
- Heart SoundsDocument56 paginiHeart SoundsBetsy Babilonia100% (1)
- Professional Plaquex InfoDocument48 paginiProfessional Plaquex Infoamelia rumenta100% (1)
- Preeclampsia NCPDocument4 paginiPreeclampsia NCPKhan Hans100% (1)
- Past Years SNQ Answer by RCSIDocument47 paginiPast Years SNQ Answer by RCSIhelamahjoubmounirdmo100% (1)
- Atrial Septal DefectDocument38 paginiAtrial Septal DefectJelita SihombingÎncă nu există evaluări
- ECG Clinical TeachingDocument21 paginiECG Clinical TeachingSumi SajiÎncă nu există evaluări
- The Heart III - Chapter 19 Case StudyDocument5 paginiThe Heart III - Chapter 19 Case StudyBrad ConnersÎncă nu există evaluări
- b4 Organisation in Animals Exam QsDocument30 paginib4 Organisation in Animals Exam QsDarius “FlawlessStreak” OpreaÎncă nu există evaluări
- Hemorrhagic Stroke: Intracerebral HemorrhageDocument5 paginiHemorrhagic Stroke: Intracerebral HemorrhagesavitageraÎncă nu există evaluări
- Blank 10Document4 paginiBlank 10Pari SharmaÎncă nu există evaluări
- The Combined Impact of Surgical Team Education and Chlorhexidine 2% Alcohol On The Reduction of Surgical Site Infection Following Cardiac SurgeryDocument7 paginiThe Combined Impact of Surgical Team Education and Chlorhexidine 2% Alcohol On The Reduction of Surgical Site Infection Following Cardiac SurgeryShandaPrimaDewiÎncă nu există evaluări
- NURS 6501 Knowledge Check: Module 5 Student Response: Scenario 1: GoutDocument16 paginiNURS 6501 Knowledge Check: Module 5 Student Response: Scenario 1: GoutBettÎncă nu există evaluări
- Pre EclampsiaDocument2 paginiPre EclampsiaDIVINA VINCEE PRESTOÎncă nu există evaluări
- Nicole Michaela Rillo Midterms Patient CaseDocument18 paginiNicole Michaela Rillo Midterms Patient CaseKyla TuanÎncă nu există evaluări
- Investigations in Oral MedicineDocument18 paginiInvestigations in Oral Medicinedr_jamal1983100% (2)
- SN02Document11 paginiSN02Enrique San NorbertoÎncă nu există evaluări
- Hesi Hints Part 4Document2 paginiHesi Hints Part 4Sharon TanveerÎncă nu există evaluări
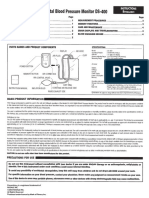
- Digital Blood Pressure Monitor DS-400: Parts Names and Product ComponentsDocument4 paginiDigital Blood Pressure Monitor DS-400: Parts Names and Product ComponentsJorÎncă nu există evaluări
- Short Cases in MedicineDocument30 paginiShort Cases in MedicineselamuÎncă nu există evaluări
- Normal Tissue Tolerance Master 11-2016Document15 paginiNormal Tissue Tolerance Master 11-2016Virgilio Rafael Tovar VasquezÎncă nu există evaluări
- Prognostic Value of Admission Blood Glucose in Diabetic and Non-Diabetic Patients With Intracerebral HemorrhageDocument7 paginiPrognostic Value of Admission Blood Glucose in Diabetic and Non-Diabetic Patients With Intracerebral HemorrhageNur Irma SafitriÎncă nu există evaluări
- Nursing Care of Patients With Digestive & Gastrointestinal DisordersDocument29 paginiNursing Care of Patients With Digestive & Gastrointestinal DisordersjoreyneeÎncă nu există evaluări
- List of VAT-Exempt ProductsDocument58 paginiList of VAT-Exempt ProductsMellinia MantesÎncă nu există evaluări
- Module 4 - Approach To The Comatose PatientDocument35 paginiModule 4 - Approach To The Comatose PatientRick RanitÎncă nu există evaluări
- Twin To Twin Transfusion PDFDocument26 paginiTwin To Twin Transfusion PDFAmbreen Z MalikÎncă nu există evaluări
- Therapeutic Indication Ofelectrohomeopathic MedicinesDocument8 paginiTherapeutic Indication Ofelectrohomeopathic MedicinesMeghanath PandhikondaÎncă nu există evaluări
- Woman Presenting with Chest PainDocument3 paginiWoman Presenting with Chest PainSteven Congress100% (1)
- Case Study 1Document3 paginiCase Study 1Da NicaÎncă nu există evaluări
- Biology Worksheet Sheep Heart DissectionDocument3 paginiBiology Worksheet Sheep Heart DissectionFluphie Bunny0% (1)