S-ar putea să vă placă și
- Ages 2 and Up - Let's Cut Paper! PDFDocument43 paginiAges 2 and Up - Let's Cut Paper! PDFRizki DwiryantiÎncă nu există evaluări
- Tanah Liat Kering / Clay 85: Macam Material (Lb/cu Yd) (%)Document1 paginăTanah Liat Kering / Clay 85: Macam Material (Lb/cu Yd) (%)Rizki DwiryantiÎncă nu există evaluări
- 10 Setting Line Alat 5: 15 GreasingDocument4 pagini10 Setting Line Alat 5: 15 GreasingRizki DwiryantiÎncă nu există evaluări
- TemplateDocument2 paginiTemplateRizki DwiryantiÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Quiz Prehist EarlyCiv 1303 Tiffany FA 23Document4 paginiQuiz Prehist EarlyCiv 1303 Tiffany FA 23dellilahking05Încă nu există evaluări
- Frog's Muscular SystemDocument9 paginiFrog's Muscular SystemRon Olegario95% (22)
- Level 2 Diploma Health and Social Care: Unit 22 - Undertake Agreed Pressure Area CareDocument6 paginiLevel 2 Diploma Health and Social Care: Unit 22 - Undertake Agreed Pressure Area CareJayne AshleyÎncă nu există evaluări
- Smart English 1 - Answer KeyDocument21 paginiSmart English 1 - Answer KeyAry SobgoÎncă nu există evaluări
- Animal ClassificationDocument4 paginiAnimal ClassificationKiyotaka BautistaÎncă nu există evaluări
- Noun Worksheet For Class 4 With Answers 1Document10 paginiNoun Worksheet For Class 4 With Answers 1Kamini jain100% (3)
- Robinson Crusoe: Zooloretto The Dice GameDocument5 paginiRobinson Crusoe: Zooloretto The Dice GameMuneeb ArshadÎncă nu există evaluări
- Anchorage Control in Bioprogressive Vs Straight-Wire Treatment PDFDocument6 paginiAnchorage Control in Bioprogressive Vs Straight-Wire Treatment PDFsolodont1Încă nu există evaluări
- Alemayehu Regassa Senbetu, EthiopiaDocument8 paginiAlemayehu Regassa Senbetu, EthiopiaAlemayehu RegassaÎncă nu există evaluări
- Impaired Physical MobilityDocument8 paginiImpaired Physical MobilityKM78% (9)
- LC4082Document3 paginiLC4082Rene NyilÎncă nu există evaluări
- Exer No. 3 - Pests of Crop Plants - Their Natural EnemiesDocument148 paginiExer No. 3 - Pests of Crop Plants - Their Natural EnemiesLuciel CypherÎncă nu există evaluări
- SN2 Jan 2007Document20 paginiSN2 Jan 2007metawarÎncă nu există evaluări
- LGBTQ Z?: Hypatia Vol. 27, No. 3 (Summer 2012) © by Hypatia, IncDocument15 paginiLGBTQ Z?: Hypatia Vol. 27, No. 3 (Summer 2012) © by Hypatia, IncSouthern PrideÎncă nu există evaluări
- Salivary Glands For BDSDocument47 paginiSalivary Glands For BDSSnighdayÎncă nu există evaluări
- Singular Answer KeyDocument2 paginiSingular Answer KeyEuclid Mark83% (6)
- 11 Axis FormationDocument61 pagini11 Axis Formationapi-3800038100% (1)
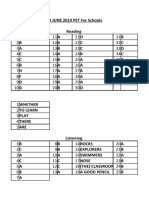
- Keys For Pet Exam PackDocument34 paginiKeys For Pet Exam PackEleftheria AggeleaÎncă nu există evaluări
- Alice Wade - Flame ThrowerDocument191 paginiAlice Wade - Flame ThrowerAnca BuzeaÎncă nu există evaluări
- TweetsDocument134 paginiTweetsAilene VasileÎncă nu există evaluări
- Pathophysiology Exam 4 - ReviewDocument18 paginiPathophysiology Exam 4 - ReviewWaqas GillÎncă nu există evaluări
- Spitz, R. A. (1955) - The Primal CavityDocument27 paginiSpitz, R. A. (1955) - The Primal CavitycabaretdadaÎncă nu există evaluări
- Tiger 3 FlashcardsDocument191 paginiTiger 3 FlashcardsEdyta SałekÎncă nu există evaluări
- Canadian Geographic Best Wildlife Photography 2018Document101 paginiCanadian Geographic Best Wildlife Photography 2018glezglez1Încă nu există evaluări
- Virus ZikaDocument2 paginiVirus Zikainta hestyaÎncă nu există evaluări
- Jolly PhonicsDocument22 paginiJolly PhonicsJack Murphy100% (2)
- Kitchen TerminologyDocument28 paginiKitchen TerminologyMariam SalongaÎncă nu există evaluări
- Tehnik - Tehnik MenjahitDocument6 paginiTehnik - Tehnik MenjahitBang mantoÎncă nu există evaluări
- Lan-Anh Bui, Josephine Wan - Amigurumi-Ingram Pub Services (2010) PDFDocument156 paginiLan-Anh Bui, Josephine Wan - Amigurumi-Ingram Pub Services (2010) PDFMarina Assa100% (1)
- GA HuntingDocument72 paginiGA HuntingEnrique HernandezÎncă nu există evaluări