S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- US Army Medical Pharmacology IDocument202 paginiUS Army Medical Pharmacology ISpace_Hulker100% (2)
- Dwarfs in Ancient EgyptDocument9 paginiDwarfs in Ancient EgyptJools GallowayÎncă nu există evaluări
- Site Master File: OF Solitaire Pharmacia PVT - LTDDocument35 paginiSite Master File: OF Solitaire Pharmacia PVT - LTDsolitairepharmacia50% (2)
- Davies - The Rock Tombs of El Amarna 03Document180 paginiDavies - The Rock Tombs of El Amarna 03Piero Pizziconi100% (1)
- Microbiological ControlDocument46 paginiMicrobiological ControlMat100% (1)
- Drugs and BruxismDocument14 paginiDrugs and BruxismAnthony HartonoÎncă nu există evaluări
- Quality Control Test of Pharmaceutical Solid Dosage FormDocument31 paginiQuality Control Test of Pharmaceutical Solid Dosage FormMoriyom Akther77% (22)
- Shirley-The Kings Physician-OConnor FestschriftDocument32 paginiShirley-The Kings Physician-OConnor FestschriftmauricioelvisÎncă nu există evaluări
- Experiential Pharmacy Practice in Institutional Pharmacy: Module 1: Part 2Document27 paginiExperiential Pharmacy Practice in Institutional Pharmacy: Module 1: Part 2levi pinedaÎncă nu există evaluări
- 1mg 1573884813954 PDFDocument2 pagini1mg 1573884813954 PDFpavan mantriÎncă nu există evaluări
- IT Pharma CompaniesDocument12 paginiIT Pharma Companiesshriya shettiwarÎncă nu există evaluări
- Drug StudyDocument41 paginiDrug StudyVecky TolentinoÎncă nu există evaluări
- Pfizer Inc.: United States Securities and Exchange CommissionDocument246 paginiPfizer Inc.: United States Securities and Exchange CommissionDipanshu NagarÎncă nu există evaluări
- Ancient Egyptian Mining ExpeditionDocument20 paginiAncient Egyptian Mining ExpeditionmauricioelvisÎncă nu există evaluări
- SJ BDJ 2009 309Document4 paginiSJ BDJ 2009 309mauricioelvisÎncă nu există evaluări
- Ancient Egypt Childbirth PracticesDocument4 paginiAncient Egypt Childbirth Practicesmauricioelvis100% (1)
- 264 2013 Article 2183Document5 pagini264 2013 Article 2183mauricioelvisÎncă nu există evaluări
- SecondTenses AfricaDocument15 paginiSecondTenses AfricamauricioelvisÎncă nu există evaluări
- Treatment Methods of Head Trauma in The Medical Papyri FinalDocument29 paginiTreatment Methods of Head Trauma in The Medical Papyri FinalmauricioelvisÎncă nu există evaluări
- Knight 2001 CircumcisionDocument23 paginiKnight 2001 CircumcisionmauricioelvisÎncă nu există evaluări
- Mental Health in The Middle East: An Egyptian PerspectiveDocument17 paginiMental Health in The Middle East: An Egyptian Perspectivemauricioelvis100% (1)
- Enamel Defects at MendesDocument13 paginiEnamel Defects at MendesmauricioelvisÎncă nu există evaluări
- Allon (LingAeg-18)Document17 paginiAllon (LingAeg-18)NivAllonÎncă nu există evaluări
- 2000 170 173 Gyory Hedvig Providing ProtectionDocument17 pagini2000 170 173 Gyory Hedvig Providing ProtectionmauricioelvisÎncă nu există evaluări
- Images of The Respiratory System in Ancient Egypt: Trachea, Bronchi and Pulmonary LobesDocument2 paginiImages of The Respiratory System in Ancient Egypt: Trachea, Bronchi and Pulmonary LobesmauricioelvisÎncă nu există evaluări
- Skeletal Health in Early Egypt MPhil Thesis Sarah MusselwhiteDocument92 paginiSkeletal Health in Early Egypt MPhil Thesis Sarah MusselwhitemauricioelvisÎncă nu există evaluări
- The Lisbon Mummy ProjectDocument12 paginiThe Lisbon Mummy Projectshailesh hari bhoiÎncă nu există evaluări
- 1 Urology in Ancient EgyptDocument1 pagină1 Urology in Ancient EgyptmauricioelvisÎncă nu există evaluări
- Treatment Methods of Head Trauma in The Medical Papyri FinalDocument29 paginiTreatment Methods of Head Trauma in The Medical Papyri FinalmauricioelvisÎncă nu există evaluări
- Thij00030 0011Document10 paginiThij00030 0011mauricioelvisÎncă nu există evaluări
- Ancient Egypt Childbirth PracticesDocument4 paginiAncient Egypt Childbirth Practicesmauricioelvis100% (1)
- HeadacheDocument6 paginiHeadachemauricioelvisÎncă nu există evaluări
- Sexuality in Ancient EgyptDocument8 paginiSexuality in Ancient EgyptmauricioelvisÎncă nu există evaluări
- SkeletalDysplasia Egypt 2008Document9 paginiSkeletalDysplasia Egypt 2008mauricioelvisÎncă nu există evaluări
- O'brien - UrologyDocument8 paginiO'brien - UrologymauricioelvisÎncă nu există evaluări
- PeasantDocument81 paginiPeasantМихаил ЧегодаевÎncă nu există evaluări
- UrologyDocument4 paginiUrologymauricioelvisÎncă nu există evaluări
- Pharmacy Management SystemDocument2 paginiPharmacy Management SystemAjay RavuriÎncă nu există evaluări
- EmulsiDocument53 paginiEmulsiYohana KedangÎncă nu există evaluări
- ATC/DDD Classification (Temporary)Document8 paginiATC/DDD Classification (Temporary)selvi aklailia rosaÎncă nu există evaluări
- PharmacologyDocument33 paginiPharmacologyYnaffit Alteza Untal100% (1)
- CHEMOTHERAPY DILUENT AND RATE GUIDEDocument3 paginiCHEMOTHERAPY DILUENT AND RATE GUIDEMohamed Abdel-AzizÎncă nu există evaluări
- Withdrawal Symptoms After Selective Serotonin Reuptake Inhibitor Discontinuation - A Systematic ReviewDocument10 paginiWithdrawal Symptoms After Selective Serotonin Reuptake Inhibitor Discontinuation - A Systematic ReviewGastón PacciaroniÎncă nu există evaluări
- Cipla Vs DR Reddy's: Financial Statement AnalysisDocument10 paginiCipla Vs DR Reddy's: Financial Statement AnalysisSrikanth Kumar KonduriÎncă nu există evaluări
- Myopia: Incidence, Pathogenesis, Management and New Possibilities of TreatmentDocument6 paginiMyopia: Incidence, Pathogenesis, Management and New Possibilities of TreatmentAl NaifÎncă nu există evaluări
- Mankind Pharma Established in 1995 With A Capital of 50 LakhsDocument8 paginiMankind Pharma Established in 1995 With A Capital of 50 LakhsJigar PriydarshiÎncă nu există evaluări
- PL - Grosir - 12-08-2023Document29 paginiPL - Grosir - 12-08-2023Fanteri Aji DharmaÎncă nu există evaluări
- InventoryDocument12 paginiInventoryMarko ParungoÎncă nu există evaluări
- Kiman PDFDocument6 paginiKiman PDFLeha QurniatiÎncă nu există evaluări
- Tertiary Hospital in Major Cities of PakistanDocument79 paginiTertiary Hospital in Major Cities of PakistanGregg AustriaÎncă nu există evaluări
- Ba-Be PDFDocument30 paginiBa-Be PDFUswatun Hasanah7201Încă nu există evaluări
- Formularium Ifrs MMB TerbaruDocument33 paginiFormularium Ifrs MMB TerbaruDesitrisnasariÎncă nu există evaluări
- Para Tram Drug StudyDocument8 paginiPara Tram Drug StudydollythesheepÎncă nu există evaluări
- Biosimilars in The Evolving Cancer Care Landscape: Experts Address Current Questions, Controversies, and Impact On Clinical PracticeDocument72 paginiBiosimilars in The Evolving Cancer Care Landscape: Experts Address Current Questions, Controversies, and Impact On Clinical PracticeNegreanu AncaÎncă nu există evaluări
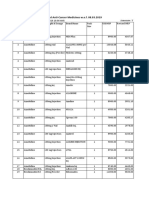
- Revised MRP of Non-Scheduled Anti-Cancer MedicinesDocument23 paginiRevised MRP of Non-Scheduled Anti-Cancer Medicinessampath seshadri100% (1)
- Pallava Template For Oral Presentation GeneralDocument20 paginiPallava Template For Oral Presentation GeneralVijay BhaskarÎncă nu există evaluări
- Sterile Product Package Integrity TestingDocument104 paginiSterile Product Package Integrity TestingJihad Elias ChahlaÎncă nu există evaluări