S-ar putea să vă placă și
- Details Pedia VitalsDocument3 paginiDetails Pedia Vitalsnikhil00007Încă nu există evaluări
- Acute Rheumatic FeverDocument39 paginiAcute Rheumatic Fevernikhil00007100% (1)
- Respiratory SystemDocument2 paginiRespiratory Systemnikhil00007Încă nu există evaluări
- Neurology HistoryDocument3 paginiNeurology Historynikhil00007Încă nu există evaluări
- CoughDocument5 paginiCoughnikhil00007Încă nu există evaluări
- Spectrum of Congenital Malformations in Newborns: in A Medical College Hospital in South IndiaDocument4 paginiSpectrum of Congenital Malformations in Newborns: in A Medical College Hospital in South Indianikhil00007Încă nu există evaluări
- History Taking and Physical Exam Checklist: Introduction To Clinical Medicine IIDocument16 paginiHistory Taking and Physical Exam Checklist: Introduction To Clinical Medicine IIYukiMaedaÎncă nu există evaluări
- CoughDocument5 paginiCoughnikhil00007Încă nu există evaluări
- Kurva TB BB 2-20 TahunDocument1 paginăKurva TB BB 2-20 Tahundibo_malmsteenÎncă nu există evaluări
- Basics of Cerebral PalsyDocument6 paginiBasics of Cerebral Palsynikhil00007Încă nu există evaluări
- Notes FeverDocument1 paginăNotes Fevernikhil00007Încă nu există evaluări
- Phenobarbitone Versus Phenytoin For Treatment of Neonatal Seizures: An Open-Label Randomized Controlled TrialDocument5 paginiPhenobarbitone Versus Phenytoin For Treatment of Neonatal Seizures: An Open-Label Randomized Controlled Trialnikhil00007Încă nu există evaluări
- Iap Immunization Guide Book 2009 2010Document180 paginiIap Immunization Guide Book 2009 2010Muralikannan Mj100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Daftar Pustaka: Universitas Sumatera UtaraDocument2 paginiDaftar Pustaka: Universitas Sumatera UtaraNavisa HaifaÎncă nu există evaluări
- 4 - 2 Not All Beta Blocker Are The Same Out With The Old, in With The New - Prof - Romdoni, FIHADocument29 pagini4 - 2 Not All Beta Blocker Are The Same Out With The Old, in With The New - Prof - Romdoni, FIHAsamuelidsÎncă nu există evaluări
- Management of Cardiogenic Shock After Acute - 2023Document10 paginiManagement of Cardiogenic Shock After Acute - 2023Angy KarakostaÎncă nu există evaluări
- Sudden Cardiac ArrestDocument1 paginăSudden Cardiac ArrestmenjahÎncă nu există evaluări
- ArrestDocument9 paginiArrestBimaIndraÎncă nu există evaluări
- Nama - Nama Peserta PRB Klinik Citra Husada No Nama No TLP Alamat DX Nama Obat Tanggal Kuttd/KetDocument4 paginiNama - Nama Peserta PRB Klinik Citra Husada No Nama No TLP Alamat DX Nama Obat Tanggal Kuttd/KetFandy HardianÎncă nu există evaluări
- Nursing Care Plan AnswerDocument6 paginiNursing Care Plan Answercoosa liquorsÎncă nu există evaluări
- Antiplatelet and Anticoagulation GuideDocument31 paginiAntiplatelet and Anticoagulation GuideMarcelliaÎncă nu există evaluări
- Sherlyn Pablo-Pablo - 2023 Senior Project Proposal FormDocument4 paginiSherlyn Pablo-Pablo - 2023 Senior Project Proposal Formapi-663260468Încă nu există evaluări
- CoronarografieDocument72 paginiCoronarografieLaurentiu AndreiÎncă nu există evaluări
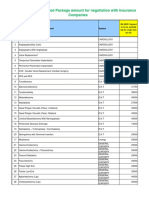
- IMA NHB Suggested Package Amount For Negotiation With Insurance CompaniesDocument5 paginiIMA NHB Suggested Package Amount For Negotiation With Insurance Companiesmonikparmar1Încă nu există evaluări
- Euad 043Document29 paginiEuad 043Pedro SeguraÎncă nu există evaluări
- Heart FailureDocument94 paginiHeart FailureAnusha Verghese100% (1)
- APPROACH TO THE PATIENT WITH CARDIOVASCULAR DISEASE-updated - 2007Document33 paginiAPPROACH TO THE PATIENT WITH CARDIOVASCULAR DISEASE-updated - 2007Malueth AnguiÎncă nu există evaluări
- Basic Life Support Techniques and ProceduresDocument7 paginiBasic Life Support Techniques and ProceduresNay ThureinÎncă nu există evaluări
- Electrocardiogram: Dr. PacnaDocument13 paginiElectrocardiogram: Dr. PacnaEcel AggasidÎncă nu există evaluări
- Differences Between ESC and ACCF/AHA STEMI GuidelinesDocument3 paginiDifferences Between ESC and ACCF/AHA STEMI GuidelinesGilbertLiemÎncă nu există evaluări
- C+F-Overview of Supraventriculer Tachycardia in Dogs and CatsDocument11 paginiC+F-Overview of Supraventriculer Tachycardia in Dogs and Catstaner_soysurenÎncă nu există evaluări
- Contoh Soal PPDS Anak (Sub Kardiologi)Document3 paginiContoh Soal PPDS Anak (Sub Kardiologi)rezkadehaÎncă nu există evaluări
- Ecg Indice 9788876407246Document12 paginiEcg Indice 9788876407246AndreaHistoryXÎncă nu există evaluări
- PacemakersDocument69 paginiPacemakersdocjeevan89100% (1)
- ECG MastersDocument644 paginiECG MastersJinnasit Tee100% (2)
- Echo Made Easy: System RequirementDocument16 paginiEcho Made Easy: System RequirementAkhi FaruqÎncă nu există evaluări
- IFU Acticor 439128-F EsDocument143 paginiIFU Acticor 439128-F EsMartin ArrietaÎncă nu există evaluări
- Family Medicine I - All Questions For Final and MidtermDocument64 paginiFamily Medicine I - All Questions For Final and Midtermzdfdgsdgsh sggaesgsÎncă nu există evaluări
- Source entry definitions provide context for medical termsDocument18 paginiSource entry definitions provide context for medical termsAnnalisa DassistiÎncă nu există evaluări
- 12 Lead ECG Color Codes 1 - 04Document62 pagini12 Lead ECG Color Codes 1 - 04ChrisieÎncă nu există evaluări
- 5 Proteze, MCCDocument82 pagini5 Proteze, MCCVlad RazvanÎncă nu există evaluări
- Cardiac Cath, Angio, Stent for CADDocument2 paginiCardiac Cath, Angio, Stent for CADIndranil SinhaÎncă nu există evaluări
- THE Electrocardiogram (ECG)Document13 paginiTHE Electrocardiogram (ECG)Bander Binjabaan Al-QahtaniÎncă nu există evaluări