S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- Irwin Rippes Intensive Care Medicine 7th Edition PDFDocument2.336 paginiIrwin Rippes Intensive Care Medicine 7th Edition PDFCristian Moldovan100% (4)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Critical Heart in Children and Infants 2019 PDFDocument1.184 paginiCritical Heart in Children and Infants 2019 PDFLiz Mtz100% (1)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Pre-Course MCQ ..................................Document1 paginăPre-Course MCQ ..................................Arslan SiddiquiÎncă nu există evaluări
- Amc Requisitioned Hospital Status 03-05-2021 5.00 PM OnlineDocument7 paginiAmc Requisitioned Hospital Status 03-05-2021 5.00 PM Onlinenaresh shahÎncă nu există evaluări
- Prevention of Central Venous Catheter-Related Bloodstream Infections: Is It Time To Add Simulation Training To The Prevention Bundle?Document6 paginiPrevention of Central Venous Catheter-Related Bloodstream Infections: Is It Time To Add Simulation Training To The Prevention Bundle?Jonatan ortizÎncă nu există evaluări
- The Use of Manual Hyperinflation in Airway Clearance: Series "Chest Physiotherapy" Edited by S.L. Hill and B. WebberDocument8 paginiThe Use of Manual Hyperinflation in Airway Clearance: Series "Chest Physiotherapy" Edited by S.L. Hill and B. WebberHello RainbowÎncă nu există evaluări
- Quality Indicators in Intensive Care Medicine For Germany Third Edition 2017Document63 paginiQuality Indicators in Intensive Care Medicine For Germany Third Edition 2017Karina AngelÎncă nu există evaluări
- Surviving Sepsis: Early Goal Directed TherapyDocument34 paginiSurviving Sepsis: Early Goal Directed Therapyyehezkiel_yesiÎncă nu există evaluări
- Aspergillus and Other Respiratory Fungal Infections in The ICU Diagnosis and Management 2018Document7 paginiAspergillus and Other Respiratory Fungal Infections in The ICU Diagnosis and Management 2018ferrevÎncă nu există evaluări
- UntitledDocument12 paginiUntitledHendra BudiantoroÎncă nu există evaluări
- Acid-Base Balance Study GuideDocument2 paginiAcid-Base Balance Study GuideNoah ClevengerÎncă nu există evaluări
- THETHESISDocument172 paginiTHETHESISAshliah Aira MarohomÎncă nu există evaluări
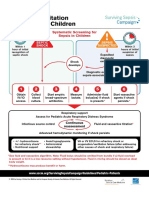
- Initial Resuscitation Algorithm For Children - Pdf.aspxDocument2 paginiInitial Resuscitation Algorithm For Children - Pdf.aspxasniatkoÎncă nu există evaluări
- Nutrition ICUDocument425 paginiNutrition ICUHELMER EMILIO PALACIOS RODRIGUEZÎncă nu există evaluări
- Career Night Booklet 2014Document85 paginiCareer Night Booklet 2014Raj PatelÎncă nu există evaluări
- Hospital PlanningDocument8 paginiHospital PlanningadithiÎncă nu există evaluări
- Sarah Brock - FinalresumetppDocument3 paginiSarah Brock - Finalresumetppapi-297710364Încă nu există evaluări
- Career Planning Guide for NursesDocument24 paginiCareer Planning Guide for NursesDhanNie CenitaÎncă nu există evaluări
- Brooke Barney: Professional DevelopmentDocument10 paginiBrooke Barney: Professional Developmentapi-405020419Încă nu există evaluări
- Sredzinski ResumeDocument2 paginiSredzinski Resumeapi-545699728Încă nu există evaluări
- 3 - PROTOCOLO (Tiene Info Importante)Document7 pagini3 - PROTOCOLO (Tiene Info Importante)KleiderAcevedoÎncă nu există evaluări
- Guía Europea DesteteDocument24 paginiGuía Europea Destetejesalo89Încă nu există evaluări
- Organization of Intensive Care UnitDocument39 paginiOrganization of Intensive Care UnitHarshil Dave100% (2)
- Introduction To Critical Care NursingDocument10 paginiIntroduction To Critical Care NursingRENEROSE TORRES0% (1)
- Course Plan For MSN-IIDocument16 paginiCourse Plan For MSN-IIRuchika KaushalÎncă nu există evaluări
- Daftar Pustaka: M. DERI RAMADHAN, Dr. Sri Setiyarini, S.KP., M.Kes Uki Noviana, S.Kep., NS., MN - SC., PH.DDocument4 paginiDaftar Pustaka: M. DERI RAMADHAN, Dr. Sri Setiyarini, S.KP., M.Kes Uki Noviana, S.Kep., NS., MN - SC., PH.DDesinta BungaÎncă nu există evaluări
- Mentoring in The Career Continuum of A Nurse: Clarifying Purpose and TimingDocument5 paginiMentoring in The Career Continuum of A Nurse: Clarifying Purpose and TimingeceÎncă nu există evaluări
- CovidPatientTreatmentGuide TFH 7-31-2021Document20 paginiCovidPatientTreatmentGuide TFH 7-31-2021Mark LaceyÎncă nu există evaluări
- Bodin Curriculum VitaeDocument8 paginiBodin Curriculum Vitaeapi-495663503Încă nu există evaluări
- Early Mobilitation For Critically Ill Patients in ICUDocument34 paginiEarly Mobilitation For Critically Ill Patients in ICUririÎncă nu există evaluări