S-ar putea să vă placă și
- Akma ResumeDocument3 paginiAkma ResumeArvenaa SubramaniamÎncă nu există evaluări
- North East Final ItineraryDocument6 paginiNorth East Final ItineraryGauravRaoÎncă nu există evaluări
- 0008Document8 pagini0008a.qawiÎncă nu există evaluări
- 5th Edition Hospital STD April 2020Document153 pagini5th Edition Hospital STD April 2020Archana GaonkarÎncă nu există evaluări
- Curriculam Vitae 1Document3 paginiCurriculam Vitae 1Rahul RajanÎncă nu există evaluări
- Reference List 1983-1995Document23 paginiReference List 1983-1995Đi Để ĐếnÎncă nu există evaluări
- CycleprocessDocument16 paginiCycleprocessGerson Antonio MocelimÎncă nu există evaluări
- Health Insurance TPA Feedback FormDocument1 paginăHealth Insurance TPA Feedback Formsubhan takildarÎncă nu există evaluări
- 9 Muharram-Ul-Haram: Office of TheDocument6 pagini9 Muharram-Ul-Haram: Office of TheEjaz AhmadÎncă nu există evaluări
- Hospital Admission ChargesDocument42 paginiHospital Admission ChargesxmancatÎncă nu există evaluări
- TTKHealthcareLimited PDFDocument60 paginiTTKHealthcareLimited PDFGururaj KoteyarÎncă nu există evaluări
- Qatar Network DatabaseDocument2 paginiQatar Network DatabaseEhab El DeenÎncă nu există evaluări
- Reimbursement Claim Form PDFDocument3 paginiReimbursement Claim Form PDFMuhammak SKÎncă nu există evaluări
- Reimbursement Claim Form (Wire Transfer)Document2 paginiReimbursement Claim Form (Wire Transfer)danigheoÎncă nu există evaluări
- AXA Non Death Claim FormDocument4 paginiAXA Non Death Claim FormKenji ChinÎncă nu există evaluări
- Claim Form: (For Reimbursement of Expenses)Document4 paginiClaim Form: (For Reimbursement of Expenses)Shankar NathÎncă nu există evaluări
- Medical Claim Reimbursement Form EnglishDocument2 paginiMedical Claim Reimbursement Form EnglishHananAhmedÎncă nu există evaluări
- Reimbursement Claim FormDocument2 paginiReimbursement Claim FormElmedina Berin HalilovićÎncă nu există evaluări
- Axa Claim FormDocument2 paginiAxa Claim FormReem Mohamed El BarraniÎncă nu există evaluări
- Appeal/Exception Request FormDocument2 paginiAppeal/Exception Request FormimranbagdadiÎncă nu există evaluări
- Non Death Claim FormDocument6 paginiNon Death Claim FormHihiÎncă nu există evaluări
- AXA Reimbursement Form ALL enDocument2 paginiAXA Reimbursement Form ALL enReynard Delos SantosÎncă nu există evaluări
- Extended Health Benefits Claim FormDocument2 paginiExtended Health Benefits Claim FormHolystreamÎncă nu există evaluări
- Claim Form en Nov 08Document4 paginiClaim Form en Nov 08Juju FernsÎncă nu există evaluări
- ADNICDocument2 paginiADNICTRTÎncă nu există evaluări
- SGP Generic Claim FormDocument5 paginiSGP Generic Claim FormSanny HamdaniÎncă nu există evaluări
- OVHC Claim Form 102017 PDFDocument3 paginiOVHC Claim Form 102017 PDFtarmudiÎncă nu există evaluări
- Put Your LOGO & SLOGAN Here: A. Policyholder - Insured DetailsDocument3 paginiPut Your LOGO & SLOGAN Here: A. Policyholder - Insured DetailsTHÍCH XEM XEÎncă nu există evaluări
- CLAIM FORM Maternity MEAF RSA 69041 3Document5 paginiCLAIM FORM Maternity MEAF RSA 69041 3Arindam ChangdarÎncă nu există evaluări
- Marsh PNG Medicare CLAIM FORMDocument3 paginiMarsh PNG Medicare CLAIM FORMKaitaMahn100% (1)
- NOW HEALTH Claim - Form - Uae - RsaDocument2 paginiNOW HEALTH Claim - Form - Uae - RsaWilliam IsaacÎncă nu există evaluări
- Claim FormDocument4 paginiClaim Formmuhammad haroonÎncă nu există evaluări
- f10 Claim FormDocument2 paginif10 Claim Formiceslurpie100% (1)
- Claim Form Dd2642Document4 paginiClaim Form Dd2642Adina BusteaÎncă nu există evaluări
- Medical Billing Process: Naveen MajetyDocument21 paginiMedical Billing Process: Naveen MajetyNaveen KumarÎncă nu există evaluări
- Reimbursement Claim Form DetailsDocument1 paginăReimbursement Claim Form DetailsJec Amrac25% (4)
- UIIC ClaimFormDocument2 paginiUIIC ClaimFormkarthikvel80Încă nu există evaluări
- UHIP Claim Form: Sun Life Assurance Company of Canada - 50150Document3 paginiUHIP Claim Form: Sun Life Assurance Company of Canada - 50150metstephÎncă nu există evaluări
- Claim Report: Travel Insurance Report FormDocument7 paginiClaim Report: Travel Insurance Report Formhoneytrap99Încă nu există evaluări
- RSPCA Vet Fee Claim Form SecuredDocument2 paginiRSPCA Vet Fee Claim Form SecuredMihaela LetÎncă nu există evaluări
- Claim Form Healthinsurance Foreign BankDocument2 paginiClaim Form Healthinsurance Foreign Banktaekyuchoi100% (1)
- Emeditek Hospital List PDFDocument20 paginiEmeditek Hospital List PDFspringsiva4497100% (4)
- Emeditek Benefit - Guide PDFDocument154 paginiEmeditek Benefit - Guide PDFShabir TrambooÎncă nu există evaluări
- Claim Form NewDocument4 paginiClaim Form Newparvazahmed03191Încă nu există evaluări
- Gulfcare Insurancec Claim FormDocument1 paginăGulfcare Insurancec Claim FormrishijaveriÎncă nu există evaluări
- Vpi FormDocument2 paginiVpi FormPadma AnneÎncă nu există evaluări
- NAS - Reimbursement Claim FormDocument2 paginiNAS - Reimbursement Claim FormPIANGO40% (5)
- OPD Claim FormDocument1 paginăOPD Claim FormKhalid SayeedÎncă nu există evaluări
- 192.168.1.206 Eclaims Cashless Viewletter - Aspx intPreIDDocument2 pagini192.168.1.206 Eclaims Cashless Viewletter - Aspx intPreIDshivamÎncă nu există evaluări
- Common PSURIClaim FormDocument5 paginiCommon PSURIClaim FormSandeep PawarÎncă nu există evaluări
- Please Update Mentioned Mobile Number As Primary Contact Details Against My Policy. I Also Hereby Confirm To Be Contacted On The Number Provided Below For Claim Status /policy RenewalDocument4 paginiPlease Update Mentioned Mobile Number As Primary Contact Details Against My Policy. I Also Hereby Confirm To Be Contacted On The Number Provided Below For Claim Status /policy RenewalSumit BhallaÎncă nu există evaluări
- GMHP Claim Form - Online PDFDocument4 paginiGMHP Claim Form - Online PDFSalem AmraneÎncă nu există evaluări
- Claim Form AOnDocument2 paginiClaim Form AOnAli Zaigham AghaÎncă nu există evaluări
- Guidelines For Reimbursement FacilityDocument2 paginiGuidelines For Reimbursement FacilityEshwar AshwathnarayanÎncă nu există evaluări
- AgreementDocument5 paginiAgreementaamir zahoorÎncă nu există evaluări
- Application For Membership Form: Application No.: Effectivity Date: Contract No.Document2 paginiApplication For Membership Form: Application No.: Effectivity Date: Contract No.Lizeth QuerubinÎncă nu există evaluări
- Assurant Health Access: in Force Underwriting Change PacketDocument10 paginiAssurant Health Access: in Force Underwriting Change PacketSwisskelly1Încă nu există evaluări
- HEALTH INSURANCE CLAIMS GUIDEDocument4 paginiHEALTH INSURANCE CLAIMS GUIDEchompiiÎncă nu există evaluări
- RE: Product: Claim Number: Incident Date:: Amex Assurance Company PO BOX 981553 EL PASO TX 79998-9920Document6 paginiRE: Product: Claim Number: Incident Date:: Amex Assurance Company PO BOX 981553 EL PASO TX 79998-9920Alexander RogersÎncă nu există evaluări
- Membership Update FormDocument4 paginiMembership Update FormbmapiraÎncă nu există evaluări
- Sample Test Building ServicesDocument2 paginiSample Test Building Servicestoalok4723Încă nu există evaluări
- CV - Alok Singh - Tech HSE & Loss Prevention Engineer (May-2018)Document5 paginiCV - Alok Singh - Tech HSE & Loss Prevention Engineer (May-2018)toalok4723Încă nu există evaluări
- Qiiita Demo EulaDocument3 paginiQiiita Demo Eulatoalok4723Încă nu există evaluări
- ZADCO Future Projects-Tenders To The Market EPC-UZ750-SUFEMS (09 01 2012)Document1 paginăZADCO Future Projects-Tenders To The Market EPC-UZ750-SUFEMS (09 01 2012)toalok4723Încă nu există evaluări
- BS en 13478 Fire Prevention and ProtectionDocument30 paginiBS en 13478 Fire Prevention and Protectiontoalok4723Încă nu există evaluări
- CV-Alok-Sr. Safety & Loss Prevention Engg (June-2015)Document5 paginiCV-Alok-Sr. Safety & Loss Prevention Engg (June-2015)toalok4723100% (1)
- H2S N TBOSIET - Alok Kumar SinghDocument2 paginiH2S N TBOSIET - Alok Kumar Singhtoalok4723Încă nu există evaluări
- CV-Alok-Sr. Safety & Loss Prevention Engg (June-2015)Document5 paginiCV-Alok-Sr. Safety & Loss Prevention Engg (June-2015)toalok4723100% (1)
- Engineering Design For Process SafetyDocument6 paginiEngineering Design For Process Safetytoalok4723Încă nu există evaluări
- Chilworth Guide To Process SafetyDocument40 paginiChilworth Guide To Process SafetyeerrddeemmÎncă nu există evaluări
- Dubai-Muscat ComparisonDocument8 paginiDubai-Muscat Comparisontoalok4723Încă nu există evaluări
- Book 1Document1 paginăBook 1toalok4723Încă nu există evaluări
- Vortex Flowmeter HTTPDocument7 paginiVortex Flowmeter HTTPtoalok4723Încă nu există evaluări
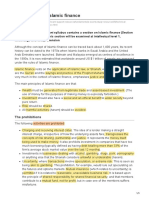
- E7 Introduction To Islamic FinanceDocument5 paginiE7 Introduction To Islamic FinanceTENGKU ANIS TENGKU YUSMAÎncă nu există evaluări
- BLP AssignmentDocument2 paginiBLP AssignmentSekar MuruganÎncă nu există evaluări
- GSM Is Abbreviation of Global System For Mobile CommunicationDocument2 paginiGSM Is Abbreviation of Global System For Mobile CommunicationPhilip Eddison PeñaflorÎncă nu există evaluări
- SEPTEMBER2023 Company (Indian and Foreign and LLP S Incorporation FO Portal ReportDocument4.027 paginiSEPTEMBER2023 Company (Indian and Foreign and LLP S Incorporation FO Portal Reportkalpana lahamageÎncă nu există evaluări
- Statement of Accountrcelispromotircppc112123032023111117Document2 paginiStatement of Accountrcelispromotircppc112123032023111117jack.rccorpÎncă nu există evaluări
- Accounts DecemberDocument28 paginiAccounts DecemberSudhan NairÎncă nu există evaluări
- FTPartnersResearch InsuranceTechnologyTrendsDocument248 paginiFTPartnersResearch InsuranceTechnologyTrendsmeÎncă nu există evaluări
- INHTA Resolution No. 01-14 Increasing Truck RatesDocument6 paginiINHTA Resolution No. 01-14 Increasing Truck RatesPortCalls80% (5)
- Customer Satisfaction Study Reliance Mutual FundsDocument2 paginiCustomer Satisfaction Study Reliance Mutual FundsebabjiÎncă nu există evaluări
- Insurance Claims BCOM 1ST YEARDocument7 paginiInsurance Claims BCOM 1ST YEARsewebib431Încă nu există evaluări
- JN0-363 (224 Questions)Document78 paginiJN0-363 (224 Questions)Sadia Baig100% (1)
- Huawei EchoLife HG8242 (GPON) Product Description (13-Jul-2012)Document16 paginiHuawei EchoLife HG8242 (GPON) Product Description (13-Jul-2012)Hernan MansillaÎncă nu există evaluări
- WWW - Bankofindia.co - in UserFiles File DebitCumATMCardApplicationDocument1 paginăWWW - Bankofindia.co - in UserFiles File DebitCumATMCardApplicationSiddharth ShanbhogueÎncă nu există evaluări
- ChallanDocument2 paginiChallanArbaaz ShaikhÎncă nu există evaluări
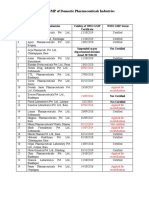
- Status of Nepali Pharma GMP CertificationDocument2 paginiStatus of Nepali Pharma GMP CertificationDapper Yourself100% (1)
- Comparative VDS TDS 2023-24 (Ammended 04 July 2023)Document12 paginiComparative VDS TDS 2023-24 (Ammended 04 July 2023)abu taher100% (2)
- New American ExpressDocument27 paginiNew American Expressamitliarliar100% (2)
- QuizletDocument4 paginiQuizletKizzea Bianca GadotÎncă nu există evaluări
- Experience Verification FormDocument1 paginăExperience Verification Formshakir ahmed0% (1)
- Customer Satisfaction in Kancheepuram 2003Document11 paginiCustomer Satisfaction in Kancheepuram 2003Shano InbarajÎncă nu există evaluări
- CA Final SFM ABC Analysis & Sure Success Strategy Nov 2023 by CADocument2 paginiCA Final SFM ABC Analysis & Sure Success Strategy Nov 2023 by CADharani SsÎncă nu există evaluări
- 033 Bob StatementDocument7 pagini033 Bob StatementSmarty Jaiswal from news of indiaÎncă nu există evaluări
- PERPETUAL INVENTORY SYSTEM - Practice SetDocument25 paginiPERPETUAL INVENTORY SYSTEM - Practice SetJAY100% (2)
- Ultimate Recurring Affiliate List - Recurring + High Ticket AffiliatesDocument3 paginiUltimate Recurring Affiliate List - Recurring + High Ticket Affiliatesebook self100% (1)
- Seat Matrix JENPAS (UG) - 2021Document4 paginiSeat Matrix JENPAS (UG) - 2021Kundan JhaÎncă nu există evaluări
- 46488c92945cff600df3a8126a600189Document3.052 pagini46488c92945cff600df3a8126a600189sandeepÎncă nu există evaluări
- Merger Analysis of HDFC and CBOPDocument18 paginiMerger Analysis of HDFC and CBOPHeidi BellÎncă nu există evaluări
- Secretary Certificate SampleDocument2 paginiSecretary Certificate SampleAngelica DaoÎncă nu există evaluări
- SG NRE Open FormDocument2 paginiSG NRE Open FormRanjith PÎncă nu există evaluări
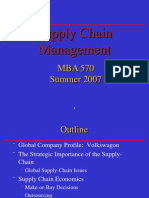
- Supply Chain Management 7Document45 paginiSupply Chain Management 7Abhi KeshwaniÎncă nu există evaluări