S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Drawing an Elephant CollaborativelyDocument17 paginiDrawing an Elephant CollaborativelyFe Canoy75% (4)
- Critical Thinking in the Classroom: Why and HowDocument41 paginiCritical Thinking in the Classroom: Why and HowIlyas El OmariÎncă nu există evaluări
- Goal Orientation TheoryDocument10 paginiGoal Orientation TheorympsbhadauriaÎncă nu există evaluări
- 20 Differentiated Instruction Strategies and ExamplesDocument19 pagini20 Differentiated Instruction Strategies and ExamplesBlessa ParagasÎncă nu există evaluări
- The Art of Problem SolvingDocument59 paginiThe Art of Problem SolvingAnubhav100% (5)
- Micro Macro TeachingDocument18 paginiMicro Macro TeachingKhor Ching100% (2)
- Unit Plan Lesson Plan 1Document5 paginiUnit Plan Lesson Plan 1api-302066692100% (1)
- Emotional IntelligenceDocument10 paginiEmotional IntelligenceAdnan PitafiÎncă nu există evaluări
- Emotional Development from Childhood to AdolescenceDocument27 paginiEmotional Development from Childhood to AdolescenceSherli PÎncă nu există evaluări
- 2016 - Why Improving and Assessing Executive Functions - Diamond PDFDocument36 pagini2016 - Why Improving and Assessing Executive Functions - Diamond PDFMADDAMÎncă nu există evaluări
- Critical Thinking Concepts and ToolsDocument9 paginiCritical Thinking Concepts and ToolsRajesh PalÎncă nu există evaluări
- AR 130 Theories of Architecture IntroductionDocument3 paginiAR 130 Theories of Architecture Introductioneyo rimasÎncă nu există evaluări
- PRINCIPLES OF TEACHING LECTURE ITEMSDocument6 paginiPRINCIPLES OF TEACHING LECTURE ITEMSDominic Dalton CalingÎncă nu există evaluări
- Portfolio in Child Adolescent and Learning PrinciplesDocument90 paginiPortfolio in Child Adolescent and Learning PrinciplesKing Louie100% (3)
- Lesson Plan HamletDocument9 paginiLesson Plan Hamletapi-347882880Încă nu există evaluări
- Ubiquitous LearningDocument60 paginiUbiquitous LearningMa Ellaine GamboaÎncă nu există evaluări
- Vroom's expectancy theoryDocument3 paginiVroom's expectancy theoryJanice Amlon100% (1)
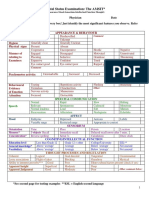
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDocument2 paginiMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- Vygotsky 1Document14 paginiVygotsky 1Princess Shiro Delos Santos100% (1)
- Learning and Development For School PersonnelDocument2 paginiLearning and Development For School PersonnelCarlos LapuzÎncă nu există evaluări
- Tonal Processing and Musical Imagery The Tonal Chronotope of MusicDocument67 paginiTonal Processing and Musical Imagery The Tonal Chronotope of MusicClaudia100% (1)
- Educ 520 - lt1 - ReflectionDocument5 paginiEduc 520 - lt1 - Reflectionapi-483914233Încă nu există evaluări
- Wozniak 1997b BehaviorismDocument14 paginiWozniak 1997b BehaviorismMariana GarcíaÎncă nu există evaluări
- Types of ObjectivesDocument9 paginiTypes of ObjectivesLuis Enrique Cornejo VargasÎncă nu există evaluări
- Constructivism: How We Build UnderstandingDocument12 paginiConstructivism: How We Build UnderstandingThanh ThanhÎncă nu există evaluări
- Expanding Your Vocabulary: Academic and Career Skills Top TipsDocument2 paginiExpanding Your Vocabulary: Academic and Career Skills Top TipsMahmoud SawabyÎncă nu există evaluări
- Environment E: Progress Monitoring & Feedback: Effective Learning Environments Observation Tool (Eleot)Document1 paginăEnvironment E: Progress Monitoring & Feedback: Effective Learning Environments Observation Tool (Eleot)Alyssa Zayas IbañezÎncă nu există evaluări
- Levels of ComprehensionDocument3 paginiLevels of ComprehensionMikaela Mae MercadoÎncă nu există evaluări
- What Is EducationDocument2 paginiWhat Is EducationYustina DianÎncă nu există evaluări
- SPEECH DELIVERY TYPES EVALUATIONDocument25 paginiSPEECH DELIVERY TYPES EVALUATIONKiervin ZapantaÎncă nu există evaluări