S-ar putea să vă placă și
- Partial Extraction Therapies (PET) Part - Maintaining Alveolar Ridge Contour at Pontic and Immediate Implant SitesDocument8 paginiPartial Extraction Therapies (PET) Part - Maintaining Alveolar Ridge Contour at Pontic and Immediate Implant SitesCristina EneÎncă nu există evaluări
- Letter To The Editor Journal Oral Implantology Regarding - Current Evidence On The Socket-ShieldDocument4 paginiLetter To The Editor Journal Oral Implantology Regarding - Current Evidence On The Socket-ShieldCristina EneÎncă nu există evaluări
- A Retrospective Evaluation of 128 Socket-Shield Cases in The Esthetic Zone and Posterior Sites - Partial Extraction Therapy With Up To 4 Years Follow-UpDocument9 paginiA Retrospective Evaluation of 128 Socket-Shield Cases in The Esthetic Zone and Posterior Sites - Partial Extraction Therapy With Up To 4 Years Follow-UpCristina EneÎncă nu există evaluări
- Letter To The Editor - Re. - The Modified Socket Shield - (J Craniofac Surg, March 2018)Document10 paginiLetter To The Editor - Re. - The Modified Socket Shield - (J Craniofac Surg, March 2018)Cristina EneÎncă nu există evaluări
- Letter To The Editor - Re. - The Modified Socket Shield - (J Craniofac Surg, March 2018)Document10 paginiLetter To The Editor - Re. - The Modified Socket Shield - (J Craniofac Surg, March 2018)Cristina EneÎncă nu există evaluări
- A Comprehensive Classification To Full ADocument14 paginiA Comprehensive Classification To Full ACristina EneÎncă nu există evaluări
- Jason Mercer Vaccinia Virus MethodsDocument318 paginiJason Mercer Vaccinia Virus MethodsCristina EneÎncă nu există evaluări
- AllergyDocument528 paginiAllergyCristina Ene100% (1)
- Fundamental of Cancer PreventionDocument10 paginiFundamental of Cancer PreventionCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument6 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Fundamentals of Cancer Prevention Part XIVDocument33 paginiFundamentals of Cancer Prevention Part XIVCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument11 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Fundamentals of Cancer Prevention Part XIIDocument22 paginiFundamentals of Cancer Prevention Part XIICristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument16 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument22 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument16 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument16 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument17 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument11 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument8 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument17 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument8 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument23 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument10 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument9 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument18 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Cardiopulmonary ResuscitationDocument16 paginiCardiopulmonary ResuscitationCristina EneÎncă nu există evaluări
- Antibiotic & Antiseptic Use in Periodontal TherapyDocument55 paginiAntibiotic & Antiseptic Use in Periodontal TherapyCristina EneÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Calculating Species Importance ValuesDocument3 paginiCalculating Species Importance Valuesabraha gebruÎncă nu există evaluări
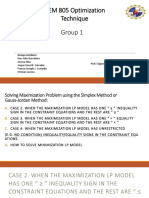
- Optimization Technique Group 1Document60 paginiOptimization Technique Group 1jmlafortezaÎncă nu există evaluări
- Digital Control Engineering 2nd Edition Fadali Solution Manual - Doc254405506Document23 paginiDigital Control Engineering 2nd Edition Fadali Solution Manual - Doc254405506chyntia50% (4)
- Dynamics of Structures Apuntes PDFDocument112 paginiDynamics of Structures Apuntes PDFHero Djoni SÎncă nu există evaluări
- JT - Installation Manual For PV Modules B1Document18 paginiJT - Installation Manual For PV Modules B1FreeLatinBird100% (1)
- Prelims Solution Ce18Document6 paginiPrelims Solution Ce18Mark Lester LualhatiÎncă nu există evaluări
- Grade 7 MathDocument3 paginiGrade 7 MathMarie Antonette SandiegoÎncă nu există evaluări
- U Center UserGuide (UBX 13005250)Document94 paginiU Center UserGuide (UBX 13005250)Phi Ra Uch100% (1)
- B8 em WavesDocument1 paginăB8 em Wavesbalikisyakubu64Încă nu există evaluări
- Neural-Network-Based Maximum Power Point Tracking Methods For Photovoltaic Systems Operating Under Fast Changing EnvironmentsDocument12 paginiNeural-Network-Based Maximum Power Point Tracking Methods For Photovoltaic Systems Operating Under Fast Changing EnvironmentsAbderrezak BadjiÎncă nu există evaluări
- Mongo DB Basic CommandsDocument15 paginiMongo DB Basic CommandsgauriÎncă nu există evaluări
- Face Mask DetectionDocument34 paginiFace Mask DetectionAmarjeet AmratÎncă nu există evaluări
- Anachem NotesDocument1 paginăAnachem NoteshÎncă nu există evaluări
- NUS Past Year PaperDocument8 paginiNUS Past Year PaperSteven KuaÎncă nu există evaluări
- Branches of Science and Sub SciencesDocument5 paginiBranches of Science and Sub SciencesSha BtstaÎncă nu există evaluări
- Operational AmplifiersDocument35 paginiOperational AmplifierskunwarÎncă nu există evaluări
- Assignment NM 2Document1 paginăAssignment NM 2Sunny KashyapÎncă nu există evaluări
- Liquid Solutions: Physical Chemistry by Prince SirDocument14 paginiLiquid Solutions: Physical Chemistry by Prince SirSunnyÎncă nu există evaluări
- Availability and ReachabilityDocument1 paginăAvailability and ReachabilityAndre Syah FahmiÎncă nu există evaluări
- Principle of StatisticsDocument6 paginiPrinciple of StatisticsMd Tarekul IslamÎncă nu există evaluări
- Economics 101: Interactive BrokersDocument11 paginiEconomics 101: Interactive BrokersDennys FreireÎncă nu există evaluări
- HW 5, 448Document16 paginiHW 5, 448pdrogos02100% (1)
- Chem 152 Lab ReportDocument21 paginiChem 152 Lab Reportapi-643022375Încă nu există evaluări
- MeDD II Calibration Guide Infusion PumpsDocument8 paginiMeDD II Calibration Guide Infusion PumpsPaulo Sanches GoncalvesÎncă nu există evaluări
- Summative Test Gr7Document1 paginăSummative Test Gr7Les Angelz100% (1)
- No Load Test: ObjectiveDocument5 paginiNo Load Test: ObjectiveyashÎncă nu există evaluări
- Module01 - AHPDocument18 paginiModule01 - AHPmia100% (1)
- Alkane and AlkeneDocument40 paginiAlkane and AlkenePawankumar Gupta91% (11)
- REVIEW TASK 1 - Capitalization, Punctuation, Fragments, Run-On Sentences and Subject & Verb Agreement Review (-1Document2 paginiREVIEW TASK 1 - Capitalization, Punctuation, Fragments, Run-On Sentences and Subject & Verb Agreement Review (-1Johao DoradoÎncă nu există evaluări
- Module One 4 BAKERY INGREDIENTSDocument46 paginiModule One 4 BAKERY INGREDIENTSIhsan BadshaÎncă nu există evaluări