S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Neinstein's Adolescent and Young Adult Health Care - A Practical Guide (6th Ed)Document2.233 paginiNeinstein's Adolescent and Young Adult Health Care - A Practical Guide (6th Ed)angelashan100% (8)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Ven ListDocument24 paginiVen ListWaf EtanoÎncă nu există evaluări
- Is Endodontic Re-Treatment Mandatory For Every Relatively Old Temporary Restoration?: A Narrative ReviewDocument7 paginiIs Endodontic Re-Treatment Mandatory For Every Relatively Old Temporary Restoration?: A Narrative ReviewARTÎncă nu există evaluări
- Airway 19 9 11Document49 paginiAirway 19 9 11SiddharthÎncă nu există evaluări
- Nursing Bullets 5Document268 paginiNursing Bullets 5kate annÎncă nu există evaluări
- Treatment Options For The Compromised Tooth - A Decision GuideDocument9 paginiTreatment Options For The Compromised Tooth - A Decision GuideARTÎncă nu există evaluări
- RO0111 00-00 WebberDocument6 paginiRO0111 00-00 WebberARTÎncă nu există evaluări
- CBCT Detection of Vertical Root Fractures JOE 2009Document4 paginiCBCT Detection of Vertical Root Fractures JOE 2009ARTÎncă nu există evaluări
- Quality Guidelines For Endodontic Treatment: Consensus Report of The European Society of EndodontologyDocument10 paginiQuality Guidelines For Endodontic Treatment: Consensus Report of The European Society of EndodontologyARTÎncă nu există evaluări
- Contemporary Endodontics - DNCADocument219 paginiContemporary Endodontics - DNCAARTÎncă nu există evaluări
- Roots 2 2010Document52 paginiRoots 2 2010ART100% (3)
- The Self-Adjusting File (SAF) - Part 3: Removal of Debris and Smear Layer-A Scanning Electron Microscope StudyDocument6 paginiThe Self-Adjusting File (SAF) - Part 3: Removal of Debris and Smear Layer-A Scanning Electron Microscope StudyARTÎncă nu există evaluări
- Roots 2 2010Document1 paginăRoots 2 2010ARTÎncă nu există evaluări
- Tapered Shaping Objectives Can Make Your Life Easier! by L. Stephen BuchananDocument7 paginiTapered Shaping Objectives Can Make Your Life Easier! by L. Stephen BuchananARTÎncă nu există evaluări
- Canal Preparation Using Only One Ni-Ti Rotary Instrument Preliminary ObservationsDocument6 paginiCanal Preparation Using Only One Ni-Ti Rotary Instrument Preliminary ObservationsARTÎncă nu există evaluări
- 681 3094 1 PBDocument9 pagini681 3094 1 PBNanis UlandariÎncă nu există evaluări
- (CPG) Philippine Guidelines On Periodic Health Examination: Screening For Neoplastic DiseasesDocument194 pagini(CPG) Philippine Guidelines On Periodic Health Examination: Screening For Neoplastic DiseasesBianca Watanabe - RatillaÎncă nu există evaluări
- Appendix #5Document14 paginiAppendix #5Euvanie Bualan RusteÎncă nu există evaluări
- InspireDocument85 paginiInspireAmit PatelÎncă nu există evaluări
- What Is Clinical Psychology?: DefinitionsDocument15 paginiWhat Is Clinical Psychology?: DefinitionsJay Mark CabreraÎncă nu există evaluări
- Florida2017 MedicalCannabisLawDocument48 paginiFlorida2017 MedicalCannabisLawTony LangeÎncă nu există evaluări
- Microstream Capnography Exercises Zoll X Series and PropaqDocument2 paginiMicrostream Capnography Exercises Zoll X Series and PropaqepraetorianÎncă nu există evaluări
- Ethical Challenges Faced by Health Care Facilities and Their StaffDocument14 paginiEthical Challenges Faced by Health Care Facilities and Their StaffAbirahÎncă nu există evaluări
- Topic 6Document27 paginiTopic 6Ayad IdresÎncă nu există evaluări
- Informative Essay On My CareerDocument5 paginiInformative Essay On My Careerapi-241280029Încă nu există evaluări
- Integrating Speech-Language Pathology Services in Palliative End-of-Life CareDocument12 paginiIntegrating Speech-Language Pathology Services in Palliative End-of-Life CareKiki PuchiÎncă nu există evaluări
- Indian Journal of Applied Basic Medical Science Sept - 2008Document28 paginiIndian Journal of Applied Basic Medical Science Sept - 2008soham2007Încă nu există evaluări
- Laboratory Activity - HIS Lab - iHOMISDocument2 paginiLaboratory Activity - HIS Lab - iHOMISFrance Cedrick RamosÎncă nu există evaluări
- ICD X Gigi Dan Mulut P Care BPJS 2019Document4 paginiICD X Gigi Dan Mulut P Care BPJS 2019puskesmassonggonÎncă nu există evaluări
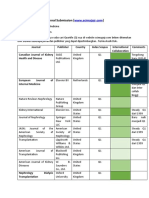
- Journal SubmissionDocument3 paginiJournal SubmissionMaruhum Bonar MarbunÎncă nu există evaluări
- Psychiatric Nursing ProcessDocument24 paginiPsychiatric Nursing ProcessJoric MagusaraÎncă nu există evaluări
- Infectious DiarrheaDocument85 paginiInfectious DiarrheaTarikÎncă nu există evaluări
- 3 Annex-G.-Draft - Profile-of-Contacts - COVID-19 PDFDocument2 pagini3 Annex-G.-Draft - Profile-of-Contacts - COVID-19 PDFErnest Jerome MalamionÎncă nu există evaluări
- Daftar PustakaDocument6 paginiDaftar Pustakayazika rimbawatiÎncă nu există evaluări
- FORMULIR RS AULIA-2Document18 paginiFORMULIR RS AULIA-2SelvyaÎncă nu există evaluări
- Context Clues Guided Reading 4.1Document4 paginiContext Clues Guided Reading 4.1Dannah SteeleÎncă nu există evaluări
- Food For Health Trends Asean Region Csiro KPMGDocument27 paginiFood For Health Trends Asean Region Csiro KPMGJassny Pey FangÎncă nu există evaluări
- Cervical Speculum ExaminationDocument41 paginiCervical Speculum ExaminationEdwin Delos Reyes AbuÎncă nu există evaluări
- Entire Infection Control Manual PDFDocument252 paginiEntire Infection Control Manual PDFAbidi HichemÎncă nu există evaluări
- Shah 2000Document4 paginiShah 2000Ardian AshadiÎncă nu există evaluări
- Lymphoma HandoutDocument5 paginiLymphoma Handoutapi-244850728Încă nu există evaluări