S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Triphasic Tactical Workout Creator Single User Powered by Sorinex EquipmentDocument50 paginiTriphasic Tactical Workout Creator Single User Powered by Sorinex EquipmentTj NewsomÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
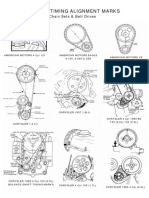
- Factory Timing Marks PDFDocument6 paginiFactory Timing Marks PDFvadiÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Houlihan Lokey IPL Valuation July 23Document35 paginiHoulihan Lokey IPL Valuation July 23Sriram Ranganathan100% (1)
- Leon Rice Flex Hitters. (C. Burns)Document6 paginiLeon Rice Flex Hitters. (C. Burns)kevmcrocker100% (1)
- Monsters - University WorksheetDocument6 paginiMonsters - University WorksheetFlorencia Cal ValenzuelaÎncă nu există evaluări
- Christopher Sommer - Basic Ring Strength DevelopmentDocument1 paginăChristopher Sommer - Basic Ring Strength Developmentjvincent6657100% (1)
- Red BullDocument15 paginiRed BullVishakha TyagiÎncă nu există evaluări
- Unit 5: Q2e Listening & Speaking 1: Audio ScriptDocument5 paginiUnit 5: Q2e Listening & Speaking 1: Audio ScriptHanaa Bin Merdah100% (1)
- Mass & Balance Exam 1Document12 paginiMass & Balance Exam 1momanbhÎncă nu există evaluări
- Fun For Movers On-Line Resources - 2017, 4th - 234pDocument234 paginiFun For Movers On-Line Resources - 2017, 4th - 234pЮлия Васильева100% (2)
- Anchor Handling Preparation Checklist300312 Rev01Document3 paginiAnchor Handling Preparation Checklist300312 Rev01Kunal Singh100% (1)
- B 8 A 00Document3 paginiB 8 A 00Stuart RodriguezÎncă nu există evaluări
- Q1. (A) Which Organ in The Body Monitors The Concentration of Glucose (Sugar) in The Blood?Document2 paginiQ1. (A) Which Organ in The Body Monitors The Concentration of Glucose (Sugar) in The Blood?DuckTalkerÎncă nu există evaluări
- P E-17Document6 paginiP E-17Rizielyn TorresÎncă nu există evaluări
- 125HBL-8-4 Parker Brass Hose BarbDocument14 pagini125HBL-8-4 Parker Brass Hose BarbMROstop.comÎncă nu există evaluări
- Pex 07 01Document6 paginiPex 07 01Stacy Cudjoe100% (1)
- Carti Bone Juice BrocherDocument4 paginiCarti Bone Juice BrocherOs MohamedÎncă nu există evaluări
- Burns - Tissue Perfusion, IneffectiveDocument3 paginiBurns - Tissue Perfusion, Ineffectivemakyofrancis20100% (1)
- 1535630-Cragacii (Elemental Shark Race) 5eDocument3 pagini1535630-Cragacii (Elemental Shark Race) 5eJeremiah HartyÎncă nu există evaluări
- Vocabulary Unit 2 3starDocument1 paginăVocabulary Unit 2 3starJose Ignacio Sierra ValverdeÎncă nu există evaluări
- Delhi Editions - Educatus Expo - 2022Document3 paginiDelhi Editions - Educatus Expo - 2022Mk GgÎncă nu există evaluări
- Management Lessons From DhoniDocument3 paginiManagement Lessons From DhonirockydondaÎncă nu există evaluări
- ClutchDocument6 paginiClutchAlex CastilloÎncă nu există evaluări
- 25 Hidden Things in Fallout 76 That Are Too Awesome For WordsDocument1 pagină25 Hidden Things in Fallout 76 That Are Too Awesome For WordsJay EsÎncă nu există evaluări
- A Groovy Kind of LoveDocument2 paginiA Groovy Kind of LovesppiderÎncă nu există evaluări
- 6.03.1 Z-Chart - Open HoleDocument2 pagini6.03.1 Z-Chart - Open HoleAdhita MeryantoÎncă nu există evaluări
- Extreme Athlete, Marshall Ulrich Is Pushing The Limits of Human Endurance (Part 1)Document1 paginăExtreme Athlete, Marshall Ulrich Is Pushing The Limits of Human Endurance (Part 1)A Distinctive StyleÎncă nu există evaluări
- BSC LifeScienceDocument29 paginiBSC LifeSciencedevil3003Încă nu există evaluări
- Level 1 Gnome ArtificerDocument3 paginiLevel 1 Gnome ArtificerLauren PolianÎncă nu există evaluări
- Fluid Mechanics - 2009Document18 paginiFluid Mechanics - 2009Paragmoni KalitaÎncă nu există evaluări