S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- IC Project Report Dashboard 10673 0Document6 paginiIC Project Report Dashboard 10673 0Anonymous Sls6WCF100% (2)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Valve & Amplifier Design, Valve EquivalentsDocument51 paginiValve & Amplifier Design, Valve EquivalentsValve Data80% (5)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- H2 Math PracticeDocument7 paginiH2 Math PracticePhoebe Heng100% (2)
- Wood Conserving StovesDocument117 paginiWood Conserving Stovesalitoparana100% (1)
- EWAD-CF EEDEN15-435 Data Books EnglishDocument42 paginiEWAD-CF EEDEN15-435 Data Books EnglishrpufitaÎncă nu există evaluări
- Beration of LightDocument7 paginiBeration of LightAnonymous i71HvPXÎncă nu există evaluări
- PDF To Image Converter v2 HOW TO USEDocument3 paginiPDF To Image Converter v2 HOW TO USEfairfaxcyclesÎncă nu există evaluări
- Dual Axis Solar Activity Tracker For Solar Panels: Department of Engineering, Sciences and Humanities (DESH)Document5 paginiDual Axis Solar Activity Tracker For Solar Panels: Department of Engineering, Sciences and Humanities (DESH)sujay patilÎncă nu există evaluări
- Access Workshop 01Document8 paginiAccess Workshop 01movogonÎncă nu există evaluări
- OL ICT First Term Kengalla Maha Vidyalaya English Medium Grade 11 MCQ Paper 2019Document5 paginiOL ICT First Term Kengalla Maha Vidyalaya English Medium Grade 11 MCQ Paper 2019mazhus123Încă nu există evaluări
- Seborg Chapter 1Document3 paginiSeborg Chapter 1maykesguerraÎncă nu există evaluări
- How Microprocessors Work PDFDocument2 paginiHow Microprocessors Work PDFdanielconstantin4Încă nu există evaluări
- 2018 06 OnlineDocument12 pagini2018 06 OnlineMohamed HasikÎncă nu există evaluări
- Ece R13Document36 paginiEce R13DilipReddiarÎncă nu există evaluări
- Sheet Pile Analysis Sheet v1.07-18.1Document2 paginiSheet Pile Analysis Sheet v1.07-18.1SES DESIGN100% (1)
- BIBLIOMETRICDocument30 paginiBIBLIOMETRICkalaranishanmuganathÎncă nu există evaluări
- Measurement of Earthing Systems: Central Networks Earthing Manual Section E4Document45 paginiMeasurement of Earthing Systems: Central Networks Earthing Manual Section E4ahmed_k7117Încă nu există evaluări
- AMC2019 StudentsResults Indonesia 8JDocument4 paginiAMC2019 StudentsResults Indonesia 8JWinety Kristiana DewiÎncă nu există evaluări
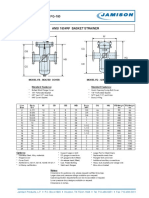
- FB-150 FQ-150 Basket StrainerDocument1 paginăFB-150 FQ-150 Basket Strainerklich77Încă nu există evaluări
- SOPRANO TIM SMTP Interface Developers GuideDocument43 paginiSOPRANO TIM SMTP Interface Developers GuidenettellectÎncă nu există evaluări
- Lab 4 SpectrophotometryDocument6 paginiLab 4 SpectrophotometryCheng FuÎncă nu există evaluări
- MAJOR14Document14 paginiMAJOR14swathi100% (1)
- AssociationBetweenBRAFV600EMutationand MortalityDocument9 paginiAssociationBetweenBRAFV600EMutationand MortalityMade RusmanaÎncă nu există evaluări
- Handwritten English Alphabet RecognitionDocument8 paginiHandwritten English Alphabet RecognitionIJRASETPublicationsÎncă nu există evaluări
- 4 Activity Guide and Evaluation Rubric - Unit 2 - Task 4 - Lets Talk and Share - Speaking Task - En.esDocument8 pagini4 Activity Guide and Evaluation Rubric - Unit 2 - Task 4 - Lets Talk and Share - Speaking Task - En.esFabiana Cataño gomezÎncă nu există evaluări
- Oracle Database 11g Transparent Data EncryptionDocument40 paginiOracle Database 11g Transparent Data EncryptionYelena BytenskayaÎncă nu există evaluări
- Technical Support Engineer - Home AssignmentDocument5 paginiTechnical Support Engineer - Home AssignmentRahul KohliÎncă nu există evaluări
- 2016 FSAE Electric Vehicle Pedal Assembly DesignDocument40 pagini2016 FSAE Electric Vehicle Pedal Assembly Designshubham rastogiÎncă nu există evaluări
- XML SerializationDocument4 paginiXML Serializationapi-3748960Încă nu există evaluări