S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Answer Sheet: First Quarter Module 9 (Lesson 2) Benefits That Cab Be Derived From Animal/Fish RaisingDocument1 paginăAnswer Sheet: First Quarter Module 9 (Lesson 2) Benefits That Cab Be Derived From Animal/Fish RaisingLorinda De Lara GonzaloÎncă nu există evaluări
- Group 2 ProteinsDocument30 paginiGroup 2 ProteinslaarnieÎncă nu există evaluări
- Oxygen Plant Project ReportDocument23 paginiOxygen Plant Project ReportAnwar Ahmad100% (1)
- Module 3Document3 paginiModule 3Cherry Ann Joy AbonÎncă nu există evaluări
- Form Cek Harga Kompetitor Des 2022 SalinanDocument24 paginiForm Cek Harga Kompetitor Des 2022 SalinanEDrian DÎncă nu există evaluări
- Nicole Erwin Professional Resume 2015-16 ClinicalDocument1 paginăNicole Erwin Professional Resume 2015-16 Clinicalapi-318488586Încă nu există evaluări
- Suguna Poultry Farm Company OverviewDocument53 paginiSuguna Poultry Farm Company OverviewShreeSharmila MurugaPrabuÎncă nu există evaluări
- Bold Crossings Excerpt Provides Insight into 19th Century MigrationDocument298 paginiBold Crossings Excerpt Provides Insight into 19th Century MigrationLanceE.OsborneÎncă nu există evaluări
- SIL (2011) List of Semantic DomainsDocument19 paginiSIL (2011) List of Semantic DomainsTakashi NakagawaÎncă nu există evaluări
- Processing of Honey A ReviewDocument19 paginiProcessing of Honey A ReviewReniÎncă nu există evaluări
- Satvic Kids BookDocument29 paginiSatvic Kids Bookmahesh gole100% (4)
- Breast GiverDocument15 paginiBreast GiverJagrit ChauhanÎncă nu există evaluări
- Cookware at Sears®: Egg Fried Rice-Easy Egg Fried Rice RecipeDocument12 paginiCookware at Sears®: Egg Fried Rice-Easy Egg Fried Rice RecipeadhimadhuÎncă nu există evaluări
- Contribution of Systems Thinking and Complex Adaptive System Attributes ToDocument11 paginiContribution of Systems Thinking and Complex Adaptive System Attributes ToIndra Yusrianto PutraÎncă nu există evaluări
- Vocabulary PracticeDocument5 paginiVocabulary PracticeValeria DonzelliÎncă nu există evaluări
- Indigenous Fermented Food and BeveragesDocument5 paginiIndigenous Fermented Food and BeveragesdodecadidoÎncă nu există evaluări
- The Asian Barbecue BookDocument181 paginiThe Asian Barbecue Bookpixtaccio100% (5)
- Chapter 15Document8 paginiChapter 15DogeTheDogÎncă nu există evaluări
- 7 Layer Cake From Petite Patisserie by Cheryl WakerhauserDocument3 pagini7 Layer Cake From Petite Patisserie by Cheryl WakerhauserAshÎncă nu există evaluări
- Feasibility Study 1 2Document9 paginiFeasibility Study 1 2Nicole TabatÎncă nu există evaluări
- Cambridge Assessment International Education: Development Studies 0453/01 October/November 2017Document11 paginiCambridge Assessment International Education: Development Studies 0453/01 October/November 2017Tee SiÎncă nu există evaluări
- Kì thi tuyển sinh lớp 10 THPT Năm 2014-2015Document8 paginiKì thi tuyển sinh lớp 10 THPT Năm 2014-2015Pluvi OphileÎncă nu există evaluări
- Houston Family of West Tennessee Cookbook & MemoirsDocument159 paginiHouston Family of West Tennessee Cookbook & MemoirsMelissa Melsa BrownÎncă nu există evaluări
- True All Undertale Text Ver.4Document143 paginiTrue All Undertale Text Ver.4CrasherGaleÎncă nu există evaluări
- Assess supplier vulnerability matrixDocument10 paginiAssess supplier vulnerability matrixNewhame Dagne100% (1)
- 40 Weird Questions To Ask Your StudentsDocument2 pagini40 Weird Questions To Ask Your Studentsanca_ramona_s100% (4)
- 11 I K S C 2018: All Questions Worth 4 PointsDocument7 pagini11 I K S C 2018: All Questions Worth 4 PointsSiscaÎncă nu există evaluări
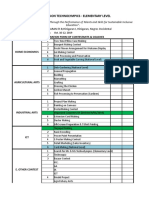
- TECHNOLYMPICSDocument2 paginiTECHNOLYMPICSArnaldo Esteves HofileñaÎncă nu există evaluări
- Delhi Airport Operator & Ground Handling ServicesDocument3 paginiDelhi Airport Operator & Ground Handling ServicesVIGNESH SELVAMÎncă nu există evaluări
- Gastronomy Tourism Events & DestinationsDocument10 paginiGastronomy Tourism Events & DestinationsRita SalibaÎncă nu există evaluări