S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Self-Myofascial Release, Purpose, Methods and TechniquesDocument47 paginiSelf-Myofascial Release, Purpose, Methods and TechniquesJonathan Warncke100% (14)
- Self-Myofascial Release, Purpose, Methods and TechniquesDocument47 paginiSelf-Myofascial Release, Purpose, Methods and TechniquesJonathan Warncke100% (14)
- Self-Myofascial Release, Purpose, Methods and TechniquesDocument47 paginiSelf-Myofascial Release, Purpose, Methods and TechniquesJonathan Warncke100% (14)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- 50 Best Calisthenic Exercises - CamEditDocument68 pagini50 Best Calisthenic Exercises - CamEditPhoenix Phoenix100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Surface AnatomyDocument63 paginiSurface AnatomyCodie SimoneauxÎncă nu există evaluări
- The 70 SbiglpDocument53 paginiThe 70 Sbiglpintensityyy100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- N O I A N: AME Rigin Nsertion Ction ErveDocument16 paginiN O I A N: AME Rigin Nsertion Ction ErveJulie Brookelle Jacquinot100% (7)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Anatomy of Upper Limb-1 EDITAN HEMATDocument49 paginiAnatomy of Upper Limb-1 EDITAN HEMATFriska Penri UtamiÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Biomechanics NotesDocument21 paginiBiomechanics Notesstarlight9394100% (1)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Bio Mechanics of The ShoulderDocument106 paginiBio Mechanics of The ShoulderOnwaree Ing100% (11)
- Slides 01 UpperLimbAnatomy PickeringDocument33 paginiSlides 01 UpperLimbAnatomy Pickeringsparta oscar100% (1)
- Color Atlas of Surgical Approaches To The Bones and Joints of The Dog and CatDocument245 paginiColor Atlas of Surgical Approaches To The Bones and Joints of The Dog and CatScott Rose100% (8)
- Bodypump: Glossary Music Express FormatsDocument40 paginiBodypump: Glossary Music Express FormatsKimberly VargasÎncă nu există evaluări
- Therapeutic Exercise MCQDocument7 paginiTherapeutic Exercise MCQNasrullah Khan73% (26)
- Stephen Hobbs - Thoracic Imaging - A Core Review-Lippincott Williams & Wilkins (2015)Document564 paginiStephen Hobbs - Thoracic Imaging - A Core Review-Lippincott Williams & Wilkins (2015)hüseyin vururÎncă nu există evaluări
- Overcoming Shoulder Impingement Syndrome, 2003Document16 paginiOvercoming Shoulder Impingement Syndrome, 2003Michelle Holman100% (1)
- Scapular Positioning in Overhead Athletes With and Without Shoulder PDFDocument10 paginiScapular Positioning in Overhead Athletes With and Without Shoulder PDFCmmb FisioterapiaÎncă nu există evaluări
- Altered Breathing Patterns During Lumbopelvic Motor ControlDocument8 paginiAltered Breathing Patterns During Lumbopelvic Motor Controlubiktrash1492Încă nu există evaluări
- Review Scapular Positioning and Movement in Unimpaired ShouldersDocument7 paginiReview Scapular Positioning and Movement in Unimpaired ShouldersCmmb FisioterapiaÎncă nu există evaluări
- Motion Analysis Study of A Scapular Orientation ExerciseDocument6 paginiMotion Analysis Study of A Scapular Orientation ExerciseCmmb FisioterapiaÎncă nu există evaluări
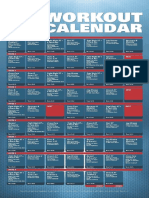
- XT2 Workout Calendar PDFDocument1 paginăXT2 Workout Calendar PDFYazmin SotoÎncă nu există evaluări
- Motor Control Retraining Exercises For Shoulder Impingement Effects On Function Muscle Activation and Biomechanics in Young AdultsDocument9 paginiMotor Control Retraining Exercises For Shoulder Impingement Effects On Function Muscle Activation and Biomechanics in Young AdultsCmmb FisioterapiaÎncă nu există evaluări
- Motion Analysis Study of A Scapular Orientation ExerciseDocument6 paginiMotion Analysis Study of A Scapular Orientation ExerciseCmmb FisioterapiaÎncă nu există evaluări
- Scapular Positioning in Overhead Athletes With and Without Shoulder PDFDocument10 paginiScapular Positioning in Overhead Athletes With and Without Shoulder PDFCmmb FisioterapiaÎncă nu există evaluări
- Altered Breathing Patterns During Lumbopelvic Motor ControlDocument8 paginiAltered Breathing Patterns During Lumbopelvic Motor Controlubiktrash1492Încă nu există evaluări
- Hurdles Performance Lead Arm Technique Advancement For Hurdle PerformanceDocument5 paginiHurdles Performance Lead Arm Technique Advancement For Hurdle PerformanceCmmb FisioterapiaÎncă nu există evaluări
- Scapular Positioning in Overhead Athletes With and Without Shoulder PDFDocument10 paginiScapular Positioning in Overhead Athletes With and Without Shoulder PDFCmmb FisioterapiaÎncă nu există evaluări
- InserviceDocument27 paginiInserviceapi-216088427Încă nu există evaluări
- Avian Skeletal System - Robert Porter PDFDocument16 paginiAvian Skeletal System - Robert Porter PDFJohn MillerÎncă nu există evaluări
- BTEC Sport - Anatomy - Muscle GroupsDocument18 paginiBTEC Sport - Anatomy - Muscle Groupsbenjenkins21Încă nu există evaluări
- Exercise 1 Frog SkeletonDocument16 paginiExercise 1 Frog SkeletonMargarette IsaacÎncă nu există evaluări
- Support Systems Grade 10Document51 paginiSupport Systems Grade 10Lance McGillÎncă nu există evaluări
- Anatomy and Physiology 6th Edition Marieb Solutions Manual Full Chapter PDFDocument41 paginiAnatomy and Physiology 6th Edition Marieb Solutions Manual Full Chapter PDFserenafinnodx100% (10)
- Acland's DVD Atlas of Human Anatomy Vol-1-TranscriptDocument36 paginiAcland's DVD Atlas of Human Anatomy Vol-1-TranscriptJaime Quimbayo EdogawaÎncă nu există evaluări
- Origo InsertioDocument7 paginiOrigo InsertioMakmur SejatiÎncă nu există evaluări
- Thoracic Incisions PDFDocument14 paginiThoracic Incisions PDFalbimar239512Încă nu există evaluări
- Cat Muscles 2Document3 paginiCat Muscles 2nathan3602Încă nu există evaluări
- 2.06 Axillary Region - Landmarks, Boundaries, Proximal Upper Limb - CirculationDocument3 pagini2.06 Axillary Region - Landmarks, Boundaries, Proximal Upper Limb - CirculationDi CanÎncă nu există evaluări
- Floating ShoulderDocument10 paginiFloating ShoulderMuhamad Amar'sÎncă nu există evaluări
- 8 - Opposite Position LoadingDocument21 pagini8 - Opposite Position Loadingbreinfout fotosÎncă nu există evaluări
- Katz Sandor enDocument49 paginiKatz Sandor enAlexÎncă nu există evaluări
- People v. Kalalo 59 PHIL 715Document10 paginiPeople v. Kalalo 59 PHIL 715AnonymousÎncă nu există evaluări
- MIDTERM - 2 - Brunnstrum - Chapter 3 Traning Procedure For The Trunk and Upper Extremity - 03-14-22Document12 paginiMIDTERM - 2 - Brunnstrum - Chapter 3 Traning Procedure For The Trunk and Upper Extremity - 03-14-22Mariane GumbanÎncă nu există evaluări
- Anatomy of CrocodilesDocument178 paginiAnatomy of CrocodilesTatenda Mageja100% (1)