Archives of Otolaryngology and Rhinology
Elena Ruz Bravo-Burguillos1*, Jose
Juan Pozo Kreilinger1, Jess Manuel
Muoz Caro3 and Antonio Ros Parra2
Department of Pathology. Hospital Universitario
La Paz. Paseo de la Castellana, 261. 28046 Madrid.
Spain
2
Department of Pathology. Hospital Universitario
Fundacin Jimnez Daz. Avda. Reyes Catlicos, 2.
28040 Madrid. Spain
3
Department of Oral and Maxillofacial Surgery.
Hospital Universitario La Paz. Paseo de la
Castellana, 261. 28046 Madrid. Spain
1
Dates: Received: 08 January, 2016; Accepted: 15
January, 2016; Published: 21 January, 2016
*Corresponding author: Elena Ruz BravoBurguillos. Department of Pathology. Hospital
Universitario La Paz. Paseo de la Castellana, 261.
28034 Madrid. Spain, Tel: +34 91 727 73 00; Fax: +34
91 727 70 49; E-mail:
www.peertechz.com
ISSN: 2455-1759
Case Report
Infant Odontogenic Myxoma: Case
Report and Literature Review of a
Specific Entity Recently Described
Abstract
Odontogenic myxomas are benign mesenchymal neoplasm most of them diagnosed in adults.
They are uncommon in the paediatric population and exceptional in infants, with only 21 cases
reported in the literature under the age of 2 years. We present a new case of infant odontogenic
myxoma, that share the same clinical and radiological presentation with the cases described in the
literature. They all presented with a painless paranasal swelling of short-term evolution, usually a
few weeks duration (while in children or adults tumours usually develop slowly) and a well-defined,
intraosseous, expansible lytic tumour of 3 cm average size in CT-scan examination. Most cases
underwent enucleation and curettage with a very low rate of recurrences (4.76%). The aim of this
article is to report a new case of this exceptional tumour, whose diagnosis was established at
histologic examination. We focus on the importance to undergo a conservative approach in this infant
population to minimize the surgical morbidity.
Keywords: Myxoma; Odontogenic tumour;
Myxomatous tumour; Maxillary tumour; Infant;
Children; Paediatric
Introduction
Odontogenic myxomas are intraosseous benign neoplasm most
of them diagnosed in adults in the third decade of life [1]. Their
frequency varies in different parts of the world between 3-20% of all
odontogenic tumours. Two thirds occur in the mandible and one
third in the maxilla, usually associated with a tooth germ. This tumour
is uncommon in the paediatric population and exceptional in infants
(under 2 years) with only 21 cases described in the literature [2].
Radiographically, this tumour is unilocular, with well-defined
and corticated borders and most of them grow slowly. As the
myxoma grows, it develops a multilocular pattern and clinically is
evident a painless swelling [1]. The larger lesions have a soap-bubble
radiographic image, similar to ameloblastoma and may present poorly
defined borders, with root displacements or periosteal reactions.
Histologically, these lesions shows randomly orientated spindle
or stellate-shaped cells set in a mucoid or myxoid matrix with a few
delicate collagen fibers [1]. The neoplasm tends to permeate into the
adjacent bony trabeculae in a pseudo-malignant pattern.
This tendency of odontogenic myxomas to permeate into marrow
spaces makes effective enucleation and curettage difficult. For small
neoplasm, aggressive curettage may be adequate, but large lesions
may require wide resection with free margins to prevent recurrences.
Recurrence rates average about 25% and usually occur during the
first 2 years after excision [1]. However, the literature review of
infant odontogenic myxomas shows a low rate of recurrences after
conservative surgery (4.76%) [2].
These tumours do not metastasize and although malignant
transformation to myxosarcoma has been reported is a rare event [3].
Case Report
A healthy 21-month-old male, with no relevant personal or family
medical history, presented to our hospital with a persistent swelling
on the right side of his face after a minor trauma a few weeks before.
The patient had persistent swelling that had no regressed. On physical
examination there was an indurated, fixed 4cm mass in his right
nasolabial groove, adjacent to the right anterior maxillary wall. The
lesion did not enlarge with crying. The overlying skin was normal.
Eye position and extra ocular motion were normal. An intraoral
examination showed obliteration of the maxillary vestibule. Clinically
the lesion looked like a mucocele.
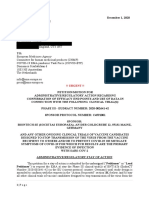
In CT-scan examination there was a low-density lesion arising
within the anterior medial aspect of the left maxillary bone with
erosion of the maxillary sinus and the lateral nasal wall (Figure 1).
There was separation of the mass from the nasal-lacrimal duct. Taking
into account the history of trauma to the area, the CT scan concluded
that the lesion was compatible with post-traumatic cyst.
Enucleation of the tumour was performed with curettage of
the surrounding bone through a vestibular incision. The patient
recovered uneventfully from surgery.
On gross pathology, the largest dimension of the lesion was 4cm
and it was gelatinous with pale brown colour. Histology revealed a
myxoid tumour with haphazardly arranged stellate to spindle-shaped
cells in a mucoid-rich intercellular matrix (Figure 2). The cells had
an eosinophilic cytoplasm, small round hyperchromatic nuclei and
fine chromatin. There was not cellular pleomorphism or nuclear
atypia. Immunohistochemical staining was positive for vimentin and
Citation: Bravo-Burguillos ER, Pozo Kreilinger JJ, Muoz Caro JM, Parra AR (2016) Infant Odontogenic Myxoma: Case Report and Literature Review of a
Specific Entity Recently Described. Arch Otolaryngol Rhinol 2(1): 006-008.
006
Bravo-Burguillos et al. (2016)
conservative surgery with only 4.76% recurrences after a follow-up
period of 3.068 years.
The histological appearance of our case is similar to those
described in the literature. These lesions resemble the mesenchymal
portion of a developing tooth. Macroscopically they are gelatinous
masses with well-defined borders but a true capsule is absent.
Microscopic examinations show a myxoid background with randomly
orientated stellate-shaped fibroblastic cells and a few delicate collagen
fibres. Some myxomas may show areas with a little more collagen
production and they are termed fibromyxomas or myxofibromas.
Binucleated cells, mild pleomorphism and mitotic figures may occur,
but these lesions do not behave differently. Immunohistochemically
tumoral cells usually react with antibodies to vimentin and musclespecific actin [1].
Figure 1: Axial CT image shows a large, unilocular and homogeneous
paranasal mass, with erosion of the maxillary antrum and the lateral nasal wall.
Figure 2: 10X HE stained tissue section of the tumor shows stellate and
spindle shape cells in a loose hypocellular myxoid stroma. In the inset HE
stained tissue section of a normal dental follicle resembling a myxoma. The
presence of peripherycally epithelial cells of the reduced enamel epithelium
exclude myxoma histologically.
the proliferation index in the MIB-1 reaction was 5%. The staining
was negative for Bcl-2, ALK1, CD31, CD34, CD68, calponin, desmin,
myogenin, smooth muscle actin and S-100. The final diagnosis was
odontogenic myxoma. The patient showed no signs of recurrence
after a follow-up period of 10 months.
Discussion
Odontogenic myxomas are considered to be benign, slowgrowing tumours that occur most commonly in the mandible
of young adults. They usually present as a slow, painless bony
expansion and radiographically, the lesion frequently appears as a
unit or multilocular radiolucency with well-defined margins [1].
To our knowledge, 21 cases have been described in infants in the
international literature [2]. All these patients, as well as our case, share
a characteristic clinical and radiological presentation. Infants (18.19
months old) present with a fixed paranasal mass (100% cases) of few
weeks evolution showing in the TC-scan a unilocular, homogeneous
lytic tumour developed from the maxilla. 71.43 % underwent
007
Myxomas are commonly associated with unerupted teeth and
probably arise from the mesenchymal portion of the tooth germ. The
histology of immature dental tissues (dental papillae and follicles)
and dental pulp is very similar to myxomas, so these structures are
the most commonly mistaken histopathologically for this tumor [4].
Dental papilla is composed of stellate and fusiform cells set in a myxoid
matrix with delicate collagen fibres. However, this tissue is always
lined, at least focally, by a rim of odontoblasts. A dental follicle can
also show a myxoid appearance. This tissue is lined along one margin
by reduced enamel epithelium (Figure 3). This features, together with
a clinical-radiologic correlation, help to distinguish these normal
dental tissues from odontogenic myxoma. Others central entities
that enters into the histological differential diagnosis are tumours
with a myxoid background: myxoid neurofibroma, chondromyxoid
fibroma, myxoid chondrosarcoma and the myxoid variant of desmoid
fibromatosis. Myxoid neurofibroma presents numerous mast cells,
a positive S-100 immunohistochemical reaction, and zones with
organization of the collagen and lesional cells into broad fascicles.
Chondromyxoid fibroma and myxoid chondrosarcoma should show
some area with chondroid differentiation and, in the latter one,
cellular atypia. The myxoid variant of desmoide fibromatosis presents
focal areas with dense collagen bundles. Cranial fasciitis can also have
a prominent myxoid background, but this is a extraosseous lesion and
express smooth muscle actin. Three cases described in the literature
were initially misdiagnosed histopathology as nodular fasciitis [2,5,6].
Treatment of this lesion consists of surgical resection, but the
extent of the resection is controversial. Some authors support a
radical surgery with wide clear margins [7,8]. However, there may
be the doubt whether to perform a wide surgical excision in children
or not, given this is a benign disease. So others authors suggest a
conservative excision or curettage [9,10]. In the series of infant
patients treated with conservative excision there is no clinical or
radiological evidence of recurrence over a median follow-up period of
3 years. These results suggest that in the infants conservative surgical
treatment is an effective therapy. The tumour is neither radiosensitive
nor chemosensitive.
As the neoplasm is located in or near the maxilla, initial clinical
misdiagnosis is not rare. Clinically differential diagnosis of a middline
mass include a wide variety of benign and malignant tumours:
encephalocele, dermoid, glioma, hamartoma, lymphangioma,
Citation: Bravo-Burguillos ER, Pozo Kreilinger JJ, Muoz Caro JM, Parra AR (2016) Infant Odontogenic Myxoma: Case Report and Literature Review of a
Specific Entity Recently Described. Arch Otolaryngol Rhinol 2(1): 006-008.
Bravo-Burguillos et al. (2016)
rhabdomiosarcoma, neurofibroma and nasolacrimal duct cyst. In our
case, the diagnosis of myxoma was not initially suggested clinically or
radiologically and a diagnosis of mucocele and post-traumatic cyst
were suggested.
This case highlights the importance of including odontogenic
myxoma in the differential diagnosis of lesions in the maxilla of
infants. The unusual clinical behaviour of this tumour as a rapidly
expansile lesion and the different entities that simule odontogenic
myxoma underline the difficulty in making a correct diagnosis, that
requires interaction among pathologist, radiologist and clinician. As
we have already discussed, review of the literature suggests that a
conservative surgery should be the initial surgical approach in infants.
References
1. Lo Muzio L, Nocini P, Favia G, Procaccini M, Mignogna MD (1996)
Odontogenic myxoma of the jaws: a clinical, radiologic, immunohistochemical,
and ultrastructural study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod
82: 426-433.
2. Kadlub N, Mbou VB, Leboulanger N, Lepointe HD, Ansari E, et al. (2014)
Infant Odontogenic Myxoma: a specific entity. J Craniomaxillofac Surg 42:
2082-2086.
3. Pahl S, Henn W, Binger T, Stein U, Remberger K (2000) Malignant
odontogenic myxoma of the maxilla: case with cytogenetic confirmation. J
Laryngol Otol 114: 533-535.
4. Suarez PA, Batsakis JG, El-Naggar AK (1996) Dont confuse dental soft
tissues with odontogenic tumors Ann Otol Rhinol Laryngol 105: 490-494.
5. James DR, Lucas VS (2014) Maxillary myxoma in a child of 11 months. A
case report. J Craniomaxillofac Surg 15: 42-44.
6. Leiberman A, Forte V, Thorner P, Crysdale W (1990) Maxillary myxoma in
children. Int J Pediatr Otorhinolaryngol 18: 277-284.
7. Prasannan L, Warren L, Herzog CE, Lopez-Camarillo L, Frankel L, et al.
(2005) Sinonasal myxoma: a pediatric case. J Pediatr Hematol Oncol 27:
90-92.
8. Iatrou IA, Theologie-Lygidakis N, Leventis MD, Michail-Strantzia C (2010)
Sinonasal myxoma in an infant. J Craniofac Surg 21: 1649-1651.
9. Rotenberg BW, Daniel SJ, Nish IA, Ngan BY, Forte V (2004) Myxomatous
lesions of the maxilla in children: a case series and review of management.
Int J Pediatr Otorhinolaryngol 68: 1251-1256.
10. Kansy K, Juergens P, Krol Z, Paulussen M, Baumhoer D, et al. (2012)
Odontogenic myxoma: diagnostic and therapeutic challenges in paediatric and
adult patients--a case series and review of the literature. J Craniomaxillofac
Surg 40: 271-276.
Copyright: 2016 Bravo-Burguillos ER, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits
unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
008
Citation: Bravo-Burguillos ER, Pozo Kreilinger JJ, Muoz Caro JM, Parra AR (2016) Infant Odontogenic Myxoma: Case Report and Literature Review of a
Specific Entity Recently Described. Arch Otolaryngol Rhinol 2(1): 006-008.
S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- BIOCHEMISTRY BOARD EXAM QUESTIONS-answersDocument7 paginiBIOCHEMISTRY BOARD EXAM QUESTIONS-answerschristinejoan100% (5)
- Genetics of RetinoblastomaDocument5 paginiGenetics of RetinoblastomadesmawitaÎncă nu există evaluări
- General Biology 2 (4 Quarter) : Animal and Plant ReproductionDocument23 paginiGeneral Biology 2 (4 Quarter) : Animal and Plant Reproductionamethyst grande100% (1)
- Book: Salt Stress in PlantsDocument517 paginiBook: Salt Stress in PlantsFrancisco Ítalo Fernandes de OliveiraÎncă nu există evaluări
- Sysmex SEED The Importance of Reticulocyte DetectionDocument8 paginiSysmex SEED The Importance of Reticulocyte DetectionGabriel J Tamayo HiguitaÎncă nu există evaluări
- Wound Healing and RepairDocument54 paginiWound Healing and RepairnyangaraÎncă nu există evaluări
- Wodarg Yeadon EMA Petition Pfizer Trial FINAL 01DEC2020 en Unsigned With ExhibitsDocument43 paginiWodarg Yeadon EMA Petition Pfizer Trial FINAL 01DEC2020 en Unsigned With ExhibitsZerohedge Janitor96% (52)
- A Survey of Solid Waste Management in Chennai (A Case Study of Around Koyambedu Market and Madhavaram Poultry Farms)Document4 paginiA Survey of Solid Waste Management in Chennai (A Case Study of Around Koyambedu Market and Madhavaram Poultry Farms)Peertechz Publications Inc.100% (1)
- Angiosarcoma of The Scalp and Face: A Hard To Treat TumorDocument4 paginiAngiosarcoma of The Scalp and Face: A Hard To Treat TumorPeertechz Publications Inc.Încă nu există evaluări
- MEK Inhibitors in Combination With Immune Checkpoint Inhibition: Should We Be Chasing Colorectal Cancer or The KRAS Mutant CancerDocument2 paginiMEK Inhibitors in Combination With Immune Checkpoint Inhibition: Should We Be Chasing Colorectal Cancer or The KRAS Mutant CancerPeertechz Publications Inc.Încă nu există evaluări
- PLGF, sFlt-1 and sFlt-1/PlGF Ratio: Promising Markers For Predicting Pre-EclampsiaDocument6 paginiPLGF, sFlt-1 and sFlt-1/PlGF Ratio: Promising Markers For Predicting Pre-EclampsiaPeertechz Publications Inc.Încă nu există evaluări
- Fishing Condition and Fishers Income: The Case of Lake Tana, EthiopiaDocument4 paginiFishing Condition and Fishers Income: The Case of Lake Tana, EthiopiaPeertechz Publications Inc.Încă nu există evaluări
- International Journal of Aquaculture and Fishery SciencesDocument4 paginiInternational Journal of Aquaculture and Fishery SciencesPeertechz Publications Inc.Încă nu există evaluări
- Imaging Journal of Clinical and Medical SciencesDocument7 paginiImaging Journal of Clinical and Medical SciencesPeertechz Publications Inc.Încă nu există evaluări
- Model Paper Government College University, FaisalabadDocument4 paginiModel Paper Government College University, FaisalabadieshrliuthlÎncă nu există evaluări
- TestBank ch01Document25 paginiTestBank ch01Edison BajramajÎncă nu există evaluări
- Molecules: The New Challenge of Green Cosmetics: Natural Food Ingredients For Cosmetic FormulationsDocument28 paginiMolecules: The New Challenge of Green Cosmetics: Natural Food Ingredients For Cosmetic FormulationsalbertoÎncă nu există evaluări
- NC-AhR Diminishes The Efficacy of Chemotherapy Via Suppressing STING Dependent Type-I Interferon in Bladder CancerDocument17 paginiNC-AhR Diminishes The Efficacy of Chemotherapy Via Suppressing STING Dependent Type-I Interferon in Bladder Cancerzhe zhÎncă nu există evaluări
- Aids 2013Document404 paginiAids 2013kovaron80Încă nu există evaluări
- Haemin Crystals LabDocument6 paginiHaemin Crystals LabNaiomiÎncă nu există evaluări
- Studentdatainterp Sexual-SelectionDocument5 paginiStudentdatainterp Sexual-SelectionParnoor SinghÎncă nu există evaluări
- Review Article On BarbituratesDocument32 paginiReview Article On BarbituratesChelsea Ritz MendozaÎncă nu există evaluări
- Name: TF Name:: LS1a Fall 2014 Lab 3 In-Lab ActivityDocument4 paginiName: TF Name:: LS1a Fall 2014 Lab 3 In-Lab ActivityThysianÎncă nu există evaluări
- The Theory of Evolution Throughout HistoryDocument18 paginiThe Theory of Evolution Throughout HistoryTupu AdreÎncă nu există evaluări
- CarbohydratesDocument3 paginiCarbohydratesmaweli09Încă nu există evaluări
- SchedulesDocument193 paginiSchedulesSuresh ParamuÎncă nu există evaluări
- Stein 2010Document5 paginiStein 2010Eunice RamosÎncă nu există evaluări
- Submitted in Partial Fulfillment of The Requirement For The Award of The Degree ofDocument47 paginiSubmitted in Partial Fulfillment of The Requirement For The Award of The Degree ofGaurav KÎncă nu există evaluări
- 6.lymphatic SysDocument43 pagini6.lymphatic SysMai Z HaniyaÎncă nu există evaluări
- Domestication Genetics WheatDocument21 paginiDomestication Genetics Wheatari novitasariÎncă nu există evaluări
- Komposisi Dan Fungsi Darah 1Document49 paginiKomposisi Dan Fungsi Darah 1Adelia MnÎncă nu există evaluări
- Philippine Medicinal Plants With Potential Immunomodulatory and ADocument19 paginiPhilippine Medicinal Plants With Potential Immunomodulatory and AJeaneteCaragÎncă nu există evaluări
- Dapi SigmaDocument2 paginiDapi SigmaeliavvÎncă nu există evaluări
- Sample - Dr. Venky's Exam Oriented Physiology - PAPER 1Document20 paginiSample - Dr. Venky's Exam Oriented Physiology - PAPER 1Jiyaa PatelÎncă nu există evaluări
- Dna FingerprintingDocument131 paginiDna FingerprintingArnen PasaribuÎncă nu există evaluări
- Cell SpecializationDocument21 paginiCell SpecializationMatt NupenÎncă nu există evaluări
- Research Project Proposals: Date PublishedDocument14 paginiResearch Project Proposals: Date PublishedJaylord AgpuldoÎncă nu există evaluări