S-ar putea să vă placă și
- Pi Is 0002937815000393Document6 paginiPi Is 0002937815000393snrarasatiÎncă nu există evaluări
- Aki 2Document6 paginiAki 2Dody Tri PermadiÎncă nu există evaluări
- Jurnal 4Document4 paginiJurnal 4Dody Tri PermadiÎncă nu există evaluări
- Diabetic Ketoacidosis: ISPAD Clinical Practice Consensus Guidelines 2006-2007Document16 paginiDiabetic Ketoacidosis: ISPAD Clinical Practice Consensus Guidelines 2006-2007ka7lonÎncă nu există evaluări
- Faktor Pencetus KadDocument7 paginiFaktor Pencetus KadDody Tri PermadiÎncă nu există evaluări
- Growth Chart For Boys Birth To 36 MonthsDocument2 paginiGrowth Chart For Boys Birth To 36 MonthsCarlos TejedaÎncă nu există evaluări
- Length and Weight For Birth To 36 Month PercentilesDocument1 paginăLength and Weight For Birth To 36 Month PercentilesEvans Oktora RolindriÎncă nu există evaluări
- Stature and Weight For 2-5 Years PercentilesDocument1 paginăStature and Weight For 2-5 Years PercentilesEvans Oktora RolindriÎncă nu există evaluări
- Head Circumferences and Weight Birth To 36 Month PercentilesDocument2 paginiHead Circumferences and Weight Birth To 36 Month PercentilesDody Tri PermadiÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Equipoise HajjajDocument4 paginiEquipoise HajjajerrelyoÎncă nu există evaluări
- The Front Desk: NABH Quality Management For Rural HospitalsDocument6 paginiThe Front Desk: NABH Quality Management For Rural HospitalsMehar AwaisÎncă nu există evaluări
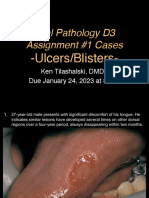
- D3 Ulcers Blisters Cases Due01242023 8amDocument13 paginiD3 Ulcers Blisters Cases Due01242023 8amLinh PhanÎncă nu există evaluări
- BSMMU Result July 2013Document33 paginiBSMMU Result July 2013Toufiq HassanÎncă nu există evaluări
- Special Report: Solutions For Joint and Arthritic Pain: by Jon Benson Author, Fit Over 40Document21 paginiSpecial Report: Solutions For Joint and Arthritic Pain: by Jon Benson Author, Fit Over 40tobyÎncă nu există evaluări
- Model State Medical Marijuana Bill PDFDocument26 paginiModel State Medical Marijuana Bill PDFJoseph PreisterÎncă nu există evaluări
- How To Calculate Calories Intake: by Group 6Document9 paginiHow To Calculate Calories Intake: by Group 6Reina Magfirah MokogintaÎncă nu există evaluări
- An Approach To Young HypertensionDocument2 paginiAn Approach To Young HypertensionNataShini RajaRatnamÎncă nu există evaluări
- Preterm LaborDocument4 paginiPreterm LaborkirbygergerÎncă nu există evaluări
- Curriculum Vitae Dr. Ari AstramDocument4 paginiCurriculum Vitae Dr. Ari AstramBedah ManadoÎncă nu există evaluări
- MKT 6080 Final Project Milestone 2 WorksheetDocument12 paginiMKT 6080 Final Project Milestone 2 WorksheetDEEÎncă nu există evaluări
- A Clinical Report On Partial Pulpotomy and Capping With Calcium Hydroxide in Permanent Incisors With Complicated Crown FractureDocument6 paginiA Clinical Report On Partial Pulpotomy and Capping With Calcium Hydroxide in Permanent Incisors With Complicated Crown Fractureroy sepÎncă nu există evaluări
- Post Term PregnancyDocument22 paginiPost Term PregnancyDarianne HernandezÎncă nu există evaluări
- Active VFC ProvidersDocument50 paginiActive VFC ProvidersClint AnthonyÎncă nu există evaluări
- Generic Name: Quinupristin/Dalfopristin - Injection (Kwin-ue-PRIS-tin/DAL-foe-PRIS-tin)Document4 paginiGeneric Name: Quinupristin/Dalfopristin - Injection (Kwin-ue-PRIS-tin/DAL-foe-PRIS-tin)Jrose CuerpoÎncă nu există evaluări
- Rights of Sewage Workers InterviewDocument8 paginiRights of Sewage Workers Interviewapi-541981758Încă nu există evaluări
- Management of Surgical UnitDocument20 paginiManagement of Surgical UnitKarrie Ann GrondinÎncă nu există evaluări
- ConnectiCare Bronze StandardDocument98 paginiConnectiCare Bronze Standardalex647Încă nu există evaluări
- Informed Consent VenipunctureDocument2 paginiInformed Consent VenipunctureBernadhita Ajuny FirdaÎncă nu există evaluări
- Medical Tourism Consultants in IndiaDocument11 paginiMedical Tourism Consultants in IndiaHealth NirvaanaÎncă nu există evaluări
- N Infection Control ManualDocument49 paginiN Infection Control ManualAnnu RajeshÎncă nu există evaluări
- E/M Audit Form: Chart #Document2 paginiE/M Audit Form: Chart #Anthony El HageÎncă nu există evaluări
- Abra (Bangued)Document3 paginiAbra (Bangued)api-251414497Încă nu există evaluări
- Terminology CHNDocument4 paginiTerminology CHNKailash NagarÎncă nu există evaluări
- Diabetic Retinopathy Screening ModuleDocument96 paginiDiabetic Retinopathy Screening ModuleSehaRizaÎncă nu există evaluări
- Reading Comprehension Exercise, May 3rdDocument3 paginiReading Comprehension Exercise, May 3rdPalupi Salwa BerliantiÎncă nu există evaluări
- Seretide Accuhaler Pi Au PDFDocument24 paginiSeretide Accuhaler Pi Au PDFJing Yi LeongÎncă nu există evaluări
- Case-Study-12 8 2Document16 paginiCase-Study-12 8 2Jaylen CayÎncă nu există evaluări
- Cashless Request FormDocument3 paginiCashless Request FormAbhineet GargÎncă nu există evaluări
- Maternal Child NursingDocument14 paginiMaternal Child NursingTina TalmadgeÎncă nu există evaluări