S-ar putea să vă placă și
- Detoxification & Chelation ProtocolsDocument213 paginiDetoxification & Chelation Protocolsdoggydog100% (3)
- USMLE Road Map ImmunologyDocument242 paginiUSMLE Road Map ImmunologyFernanda Granillo100% (9)
- Standard PrequalificationDocument67 paginiStandard PrequalificationEmmanuel Byensita67% (3)
- Pig HusbandryDocument468 paginiPig HusbandryEmmanuel Byensita100% (4)
- Pig HusbandryDocument468 paginiPig HusbandryEmmanuel Byensita100% (4)
- NLP Insider Secrets To Quickly Unleash Your Hidden PotentialDocument15 paginiNLP Insider Secrets To Quickly Unleash Your Hidden PotentialKevin ChuaÎncă nu există evaluări
- Disorders of White Blood Cells and Lymphoid TissuesDocument30 paginiDisorders of White Blood Cells and Lymphoid Tissuesammar amerÎncă nu există evaluări
- Fahim Halim Khan - Elements of Immunology-Pearson Education (2011)Document509 paginiFahim Halim Khan - Elements of Immunology-Pearson Education (2011)yusra nadeem50% (2)
- Collection, Preservation and Submission of Sample To The Microbiology LaboratoryDocument26 paginiCollection, Preservation and Submission of Sample To The Microbiology LaboratoryDrRajkumar PatelÎncă nu există evaluări
- Review Flash Card by Dr. Mitch Roy MaristelaDocument205 paginiReview Flash Card by Dr. Mitch Roy MaristelaMark Justin OcampoÎncă nu există evaluări
- Health Psychology 10th Edition Taylor Test BankDocument10 paginiHealth Psychology 10th Edition Taylor Test BankJosephJohnsonfmixo100% (15)
- Lesson Plan First AidDocument13 paginiLesson Plan First AidAlfie AyroÎncă nu există evaluări
- Infection Prevention BrochureDocument2 paginiInfection Prevention BrochureTeguh Aprian Maulana GultomÎncă nu există evaluări
- Analysis of Artificial Lift MethodsDocument32 paginiAnalysis of Artificial Lift MethodsEmmanuel ByensitaÎncă nu există evaluări
- Separator Sizing SpreadsheetDocument10 paginiSeparator Sizing SpreadsheetEmmanuel ByensitaÎncă nu există evaluări
- Separator Sizing SpreadsheetDocument10 paginiSeparator Sizing SpreadsheetEmmanuel ByensitaÎncă nu există evaluări
- Subsea Exercise No.6 PDFDocument16 paginiSubsea Exercise No.6 PDFEmmanuel Byensita100% (2)
- Related LiteratureDocument4 paginiRelated LiteratureJude FabellareÎncă nu există evaluări
- Unchangeable VedasDocument5 paginiUnchangeable VedasSon of the GodÎncă nu există evaluări
- Liquids Difference Between BuoyancyDocument28 paginiLiquids Difference Between BuoyancyabÎncă nu există evaluări
- RA ChemTech Cebu Oct2019 PDFDocument21 paginiRA ChemTech Cebu Oct2019 PDFPhilBoardResultsÎncă nu există evaluări
- Malhotra 07Document36 paginiMalhotra 07RAMEEZ. AÎncă nu există evaluări
- 6 ch3 LearnerDocument22 pagini6 ch3 Learnerapi-172952819Încă nu există evaluări
- Stop Covid-19 Genocide, Open Letter To The PresidentDocument2 paginiStop Covid-19 Genocide, Open Letter To The PresidentThe Star KenyaÎncă nu există evaluări
- POEA Block ListedDocument2 paginiPOEA Block ListedMarlon LauriagaÎncă nu există evaluări
- Finish Finish: Evidence 1 (Outline)Document11 paginiFinish Finish: Evidence 1 (Outline)Mila HashimÎncă nu există evaluări
- METC 107-S1C SyllabusDocument8 paginiMETC 107-S1C SyllabusAnonymous OPQOxbÎncă nu există evaluări
- EndosDocument8 paginiEndosAli ZainÎncă nu există evaluări
- All Washed UpDocument6 paginiAll Washed UpMia TarantoÎncă nu există evaluări
- Old English Language Beowulf in Old EnglishDocument4 paginiOld English Language Beowulf in Old Englishapi-283781689Încă nu există evaluări
- StudentsDocument1 paginăStudentsMwangi KelvinÎncă nu există evaluări
- AR: Absolute Return + Alpha. Press Release. Billion Dollar Club & Hedge Fund Report CardDocument3 paginiAR: Absolute Return + Alpha. Press Release. Billion Dollar Club & Hedge Fund Report CardAbsolute ReturnÎncă nu există evaluări
- Alignment Between Mathematics CurriculumDocument20 paginiAlignment Between Mathematics CurriculumSudheer AyazÎncă nu există evaluări
- EFL/ESL Textbook Selection in Korea and East Asia - Relevant Issues and Literature ReviewDocument11 paginiEFL/ESL Textbook Selection in Korea and East Asia - Relevant Issues and Literature ReviewWalido WilliamÎncă nu există evaluări
- Survey On CloudDocument6 paginiSurvey On CloudSatyaÎncă nu există evaluări
- Lgms Sciencefair LetterDocument1 paginăLgms Sciencefair Letterapi-292667474Încă nu există evaluări
- Nursing Assessment Tool... CardiacDocument7 paginiNursing Assessment Tool... Cardiacjai2xÎncă nu există evaluări
- BiopsyDocument5 paginiBiopsypayments8543Încă nu există evaluări
- Salman Sweets Case StudyDocument7 paginiSalman Sweets Case StudySadaqat MajeedÎncă nu există evaluări
- PanitikanDocument1 paginăPanitikanJude FabellareÎncă nu există evaluări
- Physical RestraintsDocument4 paginiPhysical RestraintsSathya PalanisamyÎncă nu există evaluări
- Assignment On Data CollectionDocument15 paginiAssignment On Data Collectiondead_fahadÎncă nu există evaluări
- Interview With Adam Zagajewski, 24 January 2003: Lance LarsenDocument10 paginiInterview With Adam Zagajewski, 24 January 2003: Lance Larsenmahesh vermaÎncă nu există evaluări
- Snake Bite ThesisDocument8 paginiSnake Bite ThesisAllison Koehn100% (2)
- 136 ZoonosesexoticosDocument7 pagini136 ZoonosesexoticosMila Fer D. PridonttÎncă nu există evaluări
- BitesDocument3 paginiBitesAmos TalsandekarÎncă nu există evaluări
- Coronavirus Crisis: Information and Help in the 2020 Pandemic - What Everyone Should KnowDe la EverandCoronavirus Crisis: Information and Help in the 2020 Pandemic - What Everyone Should KnowÎncă nu există evaluări
- Managing Stomatitis in Pet ReptilesDocument4 paginiManaging Stomatitis in Pet ReptilesPaul Jhon EugenioÎncă nu există evaluări
- Information Brochure ENDocument24 paginiInformation Brochure ENAgyei JaphineÎncă nu există evaluări
- Thesis Topics On Snake BiteDocument4 paginiThesis Topics On Snake Biteshannonsandbillings100% (2)
- Corona Virus: Information You Need and How to Protect Yourself and Your Fellow Human BeingsDe la EverandCorona Virus: Information You Need and How to Protect Yourself and Your Fellow Human BeingsÎncă nu există evaluări
- Rabies: A Case Study by Hannah IgniDocument15 paginiRabies: A Case Study by Hannah IgniHannah Clarisse Monge IgniÎncă nu există evaluări
- Top 10 Infection Prevention Questions To Ask A Nursing Home's LeadersDocument2 paginiTop 10 Infection Prevention Questions To Ask A Nursing Home's LeadersDewi RSÎncă nu există evaluări
- Chapter 18. Pinworm InfectionDocument12 paginiChapter 18. Pinworm InfectionMonica CiorneiÎncă nu există evaluări
- MRSA Consumer Factsheet BrochureDocument2 paginiMRSA Consumer Factsheet Brochurerachana.karki5431Încă nu există evaluări
- Rabies QuestionDocument4 paginiRabies QuestionRichardDumlaoÎncă nu există evaluări
- Vrts 114 - Outline of A Community Project PlanDocument11 paginiVrts 114 - Outline of A Community Project PlanClark RomandaÎncă nu există evaluări
- Earth and Life Science ReqsDocument3 paginiEarth and Life Science ReqsHazel VelascoÎncă nu există evaluări
- HIV & AIDS PreventionDocument48 paginiHIV & AIDS PreventionkiookabÎncă nu există evaluări
- NCOV Case StudyDocument3 paginiNCOV Case StudyMAC STACEY CAVEÎncă nu există evaluări
- Literature Review of Snake BiteDocument5 paginiLiterature Review of Snake Bitec5p6e5z1Încă nu există evaluări
- Barrier Nursing: Barrier Nursing Is A Largely Archaic Term For A Set of Stringent Infection ControlDocument5 paginiBarrier Nursing: Barrier Nursing Is A Largely Archaic Term For A Set of Stringent Infection ControlNrs Sani Sule MashiÎncă nu există evaluări
- The Treatment of Snake Bites in A First Aid Setting: A Systematic ReviewDocument20 paginiThe Treatment of Snake Bites in A First Aid Setting: A Systematic ReviewJohn DoeÎncă nu există evaluări
- Tropical Med Int Health - 2016 - TarantolaDocument4 paginiTropical Med Int Health - 2016 - TarantolaDeyssi Itzel Montiel BecerrilÎncă nu există evaluări
- Rabies Talking PointsDocument2 paginiRabies Talking PointsJournal StarÎncă nu există evaluări
- Frequently Asked Questions On Ebola Virus DiseaseDocument8 paginiFrequently Asked Questions On Ebola Virus DiseaseNoneyaÎncă nu există evaluări
- RabiesDocument2 paginiRabiesChhaviÎncă nu există evaluări
- CWTS2 L3 Care For HealthDocument21 paginiCWTS2 L3 Care For HealthJohn Claude TabanÎncă nu există evaluări
- Rabies ADocument26 paginiRabies ARoy BelenÎncă nu există evaluări
- Infection Control Child CareDocument1 paginăInfection Control Child CareteddwosÎncă nu există evaluări
- Enterobius Vermicularis (Pinworm) : Statpearls (Internet)Document6 paginiEnterobius Vermicularis (Pinworm) : Statpearls (Internet)Nosa MnÎncă nu există evaluări
- Stay AwayDocument16 paginiStay AwayIrfan AudahÎncă nu există evaluări
- Innes - LeprosyDocument5 paginiInnes - LeprosySzekelyÎncă nu există evaluări
- Other Factors Affecting The Emergence or Re-Emergence of Infectious DiseasesDocument15 paginiOther Factors Affecting The Emergence or Re-Emergence of Infectious DiseasesERIKA BOOTS CABALUNAÎncă nu există evaluări
- Mobile Coloring BookDocument16 paginiMobile Coloring BookEmmanuel ByensitaÎncă nu există evaluări
- Preschool ActivityDocument1 paginăPreschool ActivityEmmanuel Byensita0% (1)
- World Time ZoneMapDocument1 paginăWorld Time ZoneMapEmmanuel ByensitaÎncă nu există evaluări
- World Political MapDocument1 paginăWorld Political MapEmmanuel ByensitaÎncă nu există evaluări
- World Oceans & Seas MapDocument1 paginăWorld Oceans & Seas MapEmmanuel ByensitaÎncă nu există evaluări
- Magnetrol Level Flow Tech HandbookDocument44 paginiMagnetrol Level Flow Tech HandbookDelfinshÎncă nu există evaluări
- ULS Gasoline & Diesel Refining StudyDocument60 paginiULS Gasoline & Diesel Refining StudyEmmanuel Byensita100% (1)
- Personal Budget Planner 1Document1 paginăPersonal Budget Planner 1Emmanuel ByensitaÎncă nu există evaluări
- D4929Document8 paginiD4929Emmanuel ByensitaÎncă nu există evaluări
- How To Size A SeparatorDocument14 paginiHow To Size A SeparatorEmmanuel ByensitaÎncă nu există evaluări
- Snake Habbits & Their PreventionDocument14 paginiSnake Habbits & Their PreventionEmmanuel ByensitaÎncă nu există evaluări
- Designing An Oil & Gas SeparatorDocument2 paginiDesigning An Oil & Gas SeparatorEmmanuel ByensitaÎncă nu există evaluări
- How To Size A SeparatorDocument14 paginiHow To Size A SeparatorEmmanuel ByensitaÎncă nu există evaluări
- Handling of Petroleum Products and Their DerivativesDocument50 paginiHandling of Petroleum Products and Their DerivativesEmmanuel ByensitaÎncă nu există evaluări
- Control Methods For SnakesDocument15 paginiControl Methods For SnakesEmmanuel ByensitaÎncă nu există evaluări
- Snake Repellent - Reviews, IngredientsDocument4 paginiSnake Repellent - Reviews, IngredientsEmmanuel ByensitaÎncă nu există evaluări
- Snake Bite ManagementDocument5 paginiSnake Bite ManagementEmmanuel ByensitaÎncă nu există evaluări
- Petroleum Geology & The Exploration ProcessDocument66 paginiPetroleum Geology & The Exploration ProcessEmmanuel ByensitaÎncă nu există evaluări
- Baby TimelineDocument9 paginiBaby TimelineEmmanuel ByensitaÎncă nu există evaluări
- Case Histories, Drilling and Completion ProgramDocument8 paginiCase Histories, Drilling and Completion ProgramEmmanuel ByensitaÎncă nu există evaluări
- Oil & Gas Industry OverviewDocument98 paginiOil & Gas Industry OverviewEmmanuel ByensitaÎncă nu există evaluări
- Profession CV TamplateDocument4 paginiProfession CV TamplateEmmanuel ByensitaÎncă nu există evaluări
- Surgical TermsDocument10 paginiSurgical TermsCLaui SagibalÎncă nu există evaluări
- Chapter 8 - Transport in MammalsDocument119 paginiChapter 8 - Transport in Mammalsapi-3728508100% (1)
- Effleurage Is A Light Friction Technique Commonly Used To Begin A Massage TreatmentDocument3 paginiEffleurage Is A Light Friction Technique Commonly Used To Begin A Massage TreatmentMikki lor PuaganÎncă nu există evaluări
- BIO 230 Course Learning ObjectivesDocument21 paginiBIO 230 Course Learning ObjectivesSula GrigoreÎncă nu există evaluări
- Principles of Medical MicrobiologyDocument98 paginiPrinciples of Medical MicrobiologyJoshua MedinaÎncă nu există evaluări
- Appendix MooreDocument2 paginiAppendix Moorebrett andrea aliaÎncă nu există evaluări
- Anatomy & PhysiologyDocument11 paginiAnatomy & PhysiologyArah Lyn ApiagÎncă nu există evaluări
- HematopoiesisDocument52 paginiHematopoiesisUNO RIPPERSÎncă nu există evaluări
- CHAPTER 8 Lymphatic SystemDocument99 paginiCHAPTER 8 Lymphatic SystemAdlyn ShaheeraÎncă nu există evaluări
- Biology Form 5 Notes Chapter 1Document39 paginiBiology Form 5 Notes Chapter 1Mayghen SelvanayagamÎncă nu există evaluări
- 2017 Potts Heather CurriculumDocument120 pagini2017 Potts Heather CurriculumCyrus Flores,Încă nu există evaluări
- NCM112 Module 2 Day 2 Immune SystemDocument12 paginiNCM112 Module 2 Day 2 Immune SystemAndrea DaracanÎncă nu există evaluări
- Evolution of The Circulatory SystemDocument47 paginiEvolution of The Circulatory SystemWwwanand111Încă nu există evaluări
- Who Classification of Leukemia and Lymphoma Oct 2009shtDocument53 paginiWho Classification of Leukemia and Lymphoma Oct 2009shtBrad Weizhong Zhang100% (1)
- Bachelor of Medical Lab. Technology-BmltDocument33 paginiBachelor of Medical Lab. Technology-BmltSantosh KanelÎncă nu există evaluări
- Skims BSC Nursing Syllabus PDFDocument153 paginiSkims BSC Nursing Syllabus PDFMohd Amir Bin Bashir0% (1)
- Robbins Basic Pathology - Vinay Kumar (2017) - 198-251 PDFDocument54 paginiRobbins Basic Pathology - Vinay Kumar (2017) - 198-251 PDFMagda Tvildiani100% (1)
- Immunochemistry: Frederick A. Bettelheim William H. Brown Mary K. Campbell Shawn O. FarrellDocument41 paginiImmunochemistry: Frederick A. Bettelheim William H. Brown Mary K. Campbell Shawn O. FarrellShereen AlobinayÎncă nu există evaluări
- Organ SystemsDocument2 paginiOrgan SystemsArnel LaspinasÎncă nu există evaluări
- Krok - 1 Angliyskiy 2017Document22 paginiKrok - 1 Angliyskiy 2017ДарьяÎncă nu există evaluări
- The Following Statements Explain Why Substances Can Diffuse Easily Across The Plasma Membrane of An Amoeba, ExceptDocument10 paginiThe Following Statements Explain Why Substances Can Diffuse Easily Across The Plasma Membrane of An Amoeba, ExceptSiti Nor AishahÎncă nu există evaluări
- Anatomical Structures, Cell Types and Biomarkers of The Human Reference AtlasDocument12 paginiAnatomical Structures, Cell Types and Biomarkers of The Human Reference AtlasAnahí TessaÎncă nu există evaluări
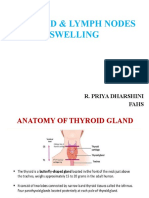
- Thyroid & Lymph NodesDocument44 paginiThyroid & Lymph NodesSarah CornerÎncă nu există evaluări