S-ar putea să vă placă și
- Beverly J. McCabe, Eric H. Frankel, Jonathan J. Wolfe Handbook of Food-Drug InteractionsDocument1 paginăBeverly J. McCabe, Eric H. Frankel, Jonathan J. Wolfe Handbook of Food-Drug Interactionsl10n_assÎncă nu există evaluări
- Classification of Cutaneous LupusDocument5 paginiClassification of Cutaneous Lupusl10n_assÎncă nu există evaluări
- Callen2009 Clinically Relevant InformationDocument4 paginiCallen2009 Clinically Relevant Informationl10n_assÎncă nu există evaluări
- F E T C: Luid AND Lectrolyte Herapy IN HildrenDocument12 paginiF E T C: Luid AND Lectrolyte Herapy IN HildrenHartantoRezaGazaliÎncă nu există evaluări
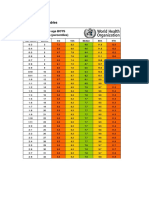
- Z Score BMI 5-19yearsold Label GirlDocument1 paginăZ Score BMI 5-19yearsold Label GirlVienny Widhyanti RosaryaÎncă nu există evaluări
- Callen2004 Update On The Management of Cutaneous Lupus ErythematosusDocument6 paginiCallen2004 Update On The Management of Cutaneous Lupus Erythematosusl10n_assÎncă nu există evaluări
- Boeck Ler 2009Document5 paginiBoeck Ler 2009l10n_assÎncă nu există evaluări
- NPPA040112 DecisiontreeDocument1 paginăNPPA040112 Decisiontreel10n_assÎncă nu există evaluări
- Wozniacka2005 Optimal Use of Antimalarials in TreatingDocument11 paginiWozniacka2005 Optimal Use of Antimalarials in Treatingl10n_assÎncă nu există evaluări
- Jurnal Kriteria Baru SleDocument10 paginiJurnal Kriteria Baru SleDr Edi HidayatÎncă nu există evaluări
- TABLE Boys 3mo To 5yr TRICEPSage PercentileDocument2 paginiTABLE Boys 3mo To 5yr TRICEPSage Percentilel10n_assÎncă nu există evaluări
- Weight gain by birth weight and age groups for boysDocument1 paginăWeight gain by birth weight and age groups for boysl10n_assÎncă nu există evaluări
- CSFDocument1 paginăCSFl10n_assÎncă nu există evaluări
- BMI Chart for Boys Ages 5-19Document1 paginăBMI Chart for Boys Ages 5-19Justitia LantuÎncă nu există evaluări
- Bmi For Age Z-ScoreDocument1 paginăBmi For Age Z-ScoreTisha Patricia OedoyÎncă nu există evaluări
- Cunnane2002 Potential Role of Polyunsaturates in Seizure Protection Achieved With The Ketogenic DietDocument5 paginiCunnane2002 Potential Role of Polyunsaturates in Seizure Protection Achieved With The Ketogenic Dietl10n_assÎncă nu există evaluări
- Bmifa Boys Z 5 19 LabelsDocument1 paginăBmifa Boys Z 5 19 LabelssufigueiraÎncă nu există evaluări
- CHT Acfa Boys Z 3 5Document1 paginăCHT Acfa Boys Z 3 5Rivadin NurwanÎncă nu există evaluări
- CSFDocument1 paginăCSFl10n_assÎncă nu există evaluări
- Temperature MeasurementDocument5 paginiTemperature Measurementl10n_ass100% (1)
- PDFDocument1 paginăPDFl10n_assÎncă nu există evaluări
- Vital Signs Reference Chart - 1Document1 paginăVital Signs Reference Chart - 1l10n_assÎncă nu există evaluări
- Lubchenco Curve PDFDocument1 paginăLubchenco Curve PDFWarren Lie25% (4)
- Dahlin2005 The Ketogenic Diet Influences The Levels of Excitatory and Inhibitory Amino Acids in The CSF in Children With Refractory EpilepsyDocument11 paginiDahlin2005 The Ketogenic Diet Influences The Levels of Excitatory and Inhibitory Amino Acids in The CSF in Children With Refractory Epilepsyl10n_assÎncă nu există evaluări
- GCS PDFDocument1 paginăGCS PDFFrincia100% (1)
- Cross2013 New Research With Diets and EpilepsyDocument6 paginiCross2013 New Research With Diets and Epilepsyl10n_assÎncă nu există evaluări
- PDFDocument1 paginăPDFl10n_assÎncă nu există evaluări
- Bough2007 Anticonvulsant Mechanisms of The Ketogenic DietDocument16 paginiBough2007 Anticonvulsant Mechanisms of The Ketogenic Dietl10n_assÎncă nu există evaluări
- Best2000 Cardiac Complications in Pediatric Patients On The Ketogenic DietDocument3 paginiBest2000 Cardiac Complications in Pediatric Patients On The Ketogenic Dietl10n_assÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Stroke Rehabilitation (PDFDrive)Document119 paginiStroke Rehabilitation (PDFDrive)Gabriela Iuliana CAZACÎncă nu există evaluări
- Normal Pressure Hydrocephalus Faqs - OriginalDocument3 paginiNormal Pressure Hydrocephalus Faqs - Originaldabell00Încă nu există evaluări
- Diagnosis and Management of Ulnar Nerve PalsyDocument20 paginiDiagnosis and Management of Ulnar Nerve PalsyamaliafarahÎncă nu există evaluări
- Lecturio Neuro Case 1Document4 paginiLecturio Neuro Case 1Danekka TanÎncă nu există evaluări
- 02 Aug14 Trans Neuro Pedia Correlates and PBL Session DrASalongaDocument3 pagini02 Aug14 Trans Neuro Pedia Correlates and PBL Session DrASalongaDelsie Vicente100% (1)
- Resume For The Post of Audiologist & Speech TherapistDocument3 paginiResume For The Post of Audiologist & Speech TherapistmathanthangaiahÎncă nu există evaluări
- Bio InvestigatoryDocument12 paginiBio InvestigatorySonakshi BadlaniÎncă nu există evaluări
- Best Neurologist in BangaloreDocument3 paginiBest Neurologist in BangaloreAlgoTrends AlgoTrendsÎncă nu există evaluări
- Febrile Seizure GuideDocument3 paginiFebrile Seizure GuideDarren Mae MosadaÎncă nu există evaluări
- Integrated Therapeutics IiiDocument82 paginiIntegrated Therapeutics IiiSalahadinÎncă nu există evaluări
- Parkinson's DiseaseDocument23 paginiParkinson's DiseaseMonika Joseph100% (1)
- Case Study 2Document2 paginiCase Study 2oumou80Încă nu există evaluări
- Approach To Space Occupying LesionDocument14 paginiApproach To Space Occupying LesionFatima JamshaidÎncă nu există evaluări
- Cerebral Palsy: Signs & Symptoms / Pathophysiology / Drug Studies / Ncps / Health TeachingsDocument22 paginiCerebral Palsy: Signs & Symptoms / Pathophysiology / Drug Studies / Ncps / Health TeachingsGeoffrey Sintaan RiveraÎncă nu există evaluări
- Autonomic HyperreflexiaDocument3 paginiAutonomic HyperreflexiaGibe BebitaÎncă nu există evaluări
- Cerebral PalsyDocument10 paginiCerebral Palsyapi-303066042Încă nu există evaluări
- Drugs in Neurology 2017Document681 paginiDrugs in Neurology 2017Roheen100% (2)
- 1961mom Wrote: On Jun 28, 2011 at 6:45amDocument6 pagini1961mom Wrote: On Jun 28, 2011 at 6:45amrobouÎncă nu există evaluări
- Developmental Milestones-Step23C 2Document20 paginiDevelopmental Milestones-Step23C 2Rob LÎncă nu există evaluări
- Congenital Malformations of The Nervous System PDFDocument16 paginiCongenital Malformations of The Nervous System PDFPriyanjali SainiÎncă nu există evaluări
- Velopharyngeal IncompetenceDocument14 paginiVelopharyngeal IncompetenceAzam M Abdullah0% (1)
- Epilepsy Guideline in AdultsDocument131 paginiEpilepsy Guideline in AdultsNEuRoLoGisT CoFFeeCuP100% (3)
- Understanding Movement DisordersDocument54 paginiUnderstanding Movement DisordersIhda ParidahÎncă nu există evaluări
- What is the nervous systemDocument12 paginiWhat is the nervous systemDietary EamcÎncă nu există evaluări
- Aaem Practice Topic in Electrodiagnostic MedicineDocument5 paginiAaem Practice Topic in Electrodiagnostic MedicineLulu LuwiiÎncă nu există evaluări
- B5W1L9.Peripheral Neuropathy - Lecture Notes 12Document4 paginiB5W1L9.Peripheral Neuropathy - Lecture Notes 12mihalcea alinÎncă nu există evaluări
- Clinical and Genetic Overview of Paroxysmal Moveme PDFDocument55 paginiClinical and Genetic Overview of Paroxysmal Moveme PDFRomy ZgheibÎncă nu există evaluări
- DAFTAR PUSTAKA EpilepsiDocument2 paginiDAFTAR PUSTAKA EpilepsiChika VithyaÎncă nu există evaluări
- Cammy Report, Ed7Document19 paginiCammy Report, Ed7Cammy Ethanei Hugo AribÎncă nu există evaluări
- Key FactsDocument3 paginiKey FactsionutmateÎncă nu există evaluări