S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Case 2 AlmostDocument8 paginiCase 2 AlmostRoberto RamosÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- History: Chief Complaint: History of Present Illness: Patient Is A 59 Year Old G6 P1051 Woman Who Is An Inmate That WasDocument9 paginiHistory: Chief Complaint: History of Present Illness: Patient Is A 59 Year Old G6 P1051 Woman Who Is An Inmate That WasRoberto RamosÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Rhie Full OcrDocument120 paginiRhie Full OcrRoberto RamosÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Case 4Document8 paginiCase 4Roberto RamosÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Universidad de Puerto Rico Mail - (No Subject)Document77 paginiUniversidad de Puerto Rico Mail - (No Subject)Roberto RamosÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Case 3Document8 paginiCase 3Roberto RamosÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Soap RoutineDocument3 paginiSoap RoutineRoberto Ramos100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- McCowan SGA RiskFactors BJOG 2010Document9 paginiMcCowan SGA RiskFactors BJOG 2010Roberto RamosÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Long Case Presentation FINAL-33Document7 paginiLong Case Presentation FINAL-33Roberto RamosÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Paciente 3Document80 paginiPaciente 3Roberto RamosÎncă nu există evaluări
- Long Case Presentation FINAL-5Document7 paginiLong Case Presentation FINAL-5Roberto RamosÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Long Case Presentation FINAL-5Document7 paginiLong Case Presentation FINAL-5Roberto RamosÎncă nu există evaluări
- Radio ObGynDocument1 paginăRadio ObGynRoberto RamosÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- "Repaso" Shelf OB - GYN 2 2Document9 pagini"Repaso" Shelf OB - GYN 2 2Roberto RamosÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Universidad Puerto Rico Manual 1415Document161 paginiUniversidad Puerto Rico Manual 1415Roberto RamosÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Repaso ShelfDocument135 paginiRepaso ShelfRoberto RamosÎncă nu există evaluări
- Untitled Spreadsheet 2Document4 paginiUntitled Spreadsheet 2Roberto RamosÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Progress Note Osce - HIV (1) - 2Document1 paginăProgress Note Osce - HIV (1) - 2Roberto RamosÎncă nu există evaluări
- HTTPDocument1 paginăHTTPRoberto RamosÎncă nu există evaluări
- Final - Answers of Ekg QuizDocument46 paginiFinal - Answers of Ekg QuizRoberto RamosÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- SEPSIS Case 2014 - August-2Document45 paginiSEPSIS Case 2014 - August-2Roberto RamosÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- DR - Umpierrere2012 2013 4Document70 paginiDR - Umpierrere2012 2013 4Roberto RamosÎncă nu există evaluări
- Health Maintenance Cases For Discussion-5Document4 paginiHealth Maintenance Cases For Discussion-5Roberto RamosÎncă nu există evaluări
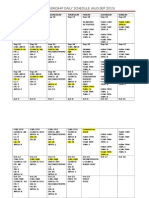
- Ob-Gyn Clerkship Daily Schedule (Aug-Sep 2015)Document3 paginiOb-Gyn Clerkship Daily Schedule (Aug-Sep 2015)Roberto RamosÎncă nu există evaluări
- There Is Been An Overlooked But Important TopicDocument2 paginiThere Is Been An Overlooked But Important TopicRoberto RamosÎncă nu există evaluări
- HTTPDocument1 paginăHTTPRoberto RamosÎncă nu există evaluări
- There Is Been An Overlooked But Important TopicDocument2 paginiThere Is Been An Overlooked But Important TopicRoberto RamosÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Thales Journal Club EsawyerDocument6 paginiThales Journal Club Esawyerapi-535001113Încă nu există evaluări
- Deborah Falla The Role of Motor Learning and Neuroplasticity in Designing RehabilitationDocument5 paginiDeborah Falla The Role of Motor Learning and Neuroplasticity in Designing RehabilitationDago Angel Prieto PalavecinoÎncă nu există evaluări
- Getting Past Your BreakupDocument4 paginiGetting Past Your BreakupKrish Malhotra0% (1)
- Tips and Practical Plasma Applications.FDocument45 paginiTips and Practical Plasma Applications.FSorin RotaruÎncă nu există evaluări
- How Can Holistic Health Benefit MeDocument2 paginiHow Can Holistic Health Benefit Meanna ticaÎncă nu există evaluări
- Billroth II ProcedureDocument2 paginiBillroth II ProcedureJasmin MirandaÎncă nu există evaluări
- Renal Diseases " Review "Document22 paginiRenal Diseases " Review "api-3827876Încă nu există evaluări
- Executive SummaryPOWER PIONTDocument12 paginiExecutive SummaryPOWER PIONTXha LomerioÎncă nu există evaluări
- Bali Cyclosporine Reduces Sclerosis in (Morphea, Systemic Sclerosis)Document8 paginiBali Cyclosporine Reduces Sclerosis in (Morphea, Systemic Sclerosis)Azmi FadhlihÎncă nu există evaluări
- Homoeopathy Shoots The Shooting Pain (A Case of Trigeminal Neuralgia Treated at Ber Sarai Dispensary)Document14 paginiHomoeopathy Shoots The Shooting Pain (A Case of Trigeminal Neuralgia Treated at Ber Sarai Dispensary)Homoeopathic Pulse100% (1)
- Peripheral Vascular Disease NursingDocument13 paginiPeripheral Vascular Disease NursingCatlyn Chatpman100% (1)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- 426 C1 OsceDocument21 pagini426 C1 Osceaini natashaÎncă nu există evaluări
- Pyelonephritis 1 Running Head: PYELONEPHRITISDocument4 paginiPyelonephritis 1 Running Head: PYELONEPHRITISEÎncă nu există evaluări
- AssertivenessDocument4 paginiAssertivenessDamir MujagicÎncă nu există evaluări
- Counselling-GATHER ApproachDocument23 paginiCounselling-GATHER ApproachAnilkumar JaraliÎncă nu există evaluări
- The Biopsychosocial Formulation Manual A Guide For Mental Health Professionals PDFDocument178 paginiThe Biopsychosocial Formulation Manual A Guide For Mental Health Professionals PDFLeidy Yiseth Cárdenas100% (4)
- Acrylic Removable Partial Denture & Impression Techniques in Complete DentureDocument9 paginiAcrylic Removable Partial Denture & Impression Techniques in Complete DentureMohammed ZiaÎncă nu există evaluări
- Application of CTASDocument32 paginiApplication of CTASsidekick941Încă nu există evaluări
- Resorption of A Calcium Hydroxide/iodoform Paste (Vitapex) in Root Canal Therapy For Primary Teeth: A Case ReportDocument4 paginiResorption of A Calcium Hydroxide/iodoform Paste (Vitapex) in Root Canal Therapy For Primary Teeth: A Case ReportHasbi Brilian KumaraÎncă nu există evaluări
- Nursing Care Plan For Mother:: Sno Assessment Diagnosis Planning Implementation EvaluationDocument4 paginiNursing Care Plan For Mother:: Sno Assessment Diagnosis Planning Implementation Evaluationmishti100% (1)
- Ocular TherapeuticsDocument1 paginăOcular TherapeuticsNikka ReyesÎncă nu există evaluări
- Ace InhibitorsDocument15 paginiAce InhibitorsCarolyn Conn EdwardsÎncă nu există evaluări
- Monkey Drug TrialDocument5 paginiMonkey Drug TrialFelipe KawashiroÎncă nu există evaluări
- The Psychological AspectsDocument7 paginiThe Psychological AspectsInvisible_TouchÎncă nu există evaluări
- Evolutionary Theory and Cognitive Therapy PDFDocument2 paginiEvolutionary Theory and Cognitive Therapy PDFDeniseÎncă nu există evaluări
- BrochureDocument2 paginiBrochureapi-375895852Încă nu există evaluări
- Management of TMDDocument22 paginiManagement of TMDWallisson SoaresÎncă nu există evaluări
- In Vivo Dosimetry in BrachytherapyDocument17 paginiIn Vivo Dosimetry in BrachytherapySUBHAÎncă nu există evaluări
- Motivational Enhancement TherapyDocument9 paginiMotivational Enhancement TherapyDavid Alejandro VilledaÎncă nu există evaluări
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (24)