S-ar putea să vă placă și
- Diabetic Foot Risks and ComplicationsDocument98 paginiDiabetic Foot Risks and ComplicationsRashed ShatnawiÎncă nu există evaluări
- Diabetic Foot Complications GuideDocument26 paginiDiabetic Foot Complications Guideili_izyan100% (1)
- Sps 23132Document9 paginiSps 23132TrioRWicaksanaÎncă nu există evaluări
- FinalDocument87 paginiFinalSanjiv GoyalÎncă nu există evaluări
- Hypocalcemia - Diagnosis and Treatment - Endotext - NCBI BookshelfDocument31 paginiHypocalcemia - Diagnosis and Treatment - Endotext - NCBI Bookshelfgalnaresdaniela7Încă nu există evaluări
- Disease of Skeletal Muscle and JointsDocument7 paginiDisease of Skeletal Muscle and JointsNur Amirah FarhanahÎncă nu există evaluări
- A Review of The Pa Tho PhysiologyDocument7 paginiA Review of The Pa Tho Physiologyintan_mgÎncă nu există evaluări
- Genetik Basis of Disorder in Orthopaedics AlvianDocument53 paginiGenetik Basis of Disorder in Orthopaedics AlvianAlvian AdriyantoÎncă nu există evaluări
- Labovitz2019 PDFDocument19 paginiLabovitz2019 PDFArthur TeixeiraÎncă nu există evaluări
- Chronic Kidney Disease (CKD) - McMaster Pathophysiology ReviewDocument5 paginiChronic Kidney Disease (CKD) - McMaster Pathophysiology ReviewAnonymous uziTjed5j100% (1)
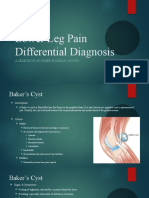
- Lower Leg Pain Differential Diagnosis - OtherDocument13 paginiLower Leg Pain Differential Diagnosis - Otherapi-619359087Încă nu există evaluări
- MSK Pathology For USMLE Step OneDocument6 paginiMSK Pathology For USMLE Step OneGrilled CroweÎncă nu există evaluări
- The Diabetic Foot: (Physician'S Overview)Document43 paginiThe Diabetic Foot: (Physician'S Overview)Imtiaz AhmedÎncă nu există evaluări
- Methods of Improving The Treatment and Prevention of Patients With Diabetic Foot SyndromeDocument7 paginiMethods of Improving The Treatment and Prevention of Patients With Diabetic Foot SyndromeCentral Asian StudiesÎncă nu există evaluări
- Charcot Neuropathy TBH PresentationDocument15 paginiCharcot Neuropathy TBH PresentationHuguette Marie NseleÎncă nu există evaluări
- Diabetic FootDocument31 paginiDiabetic FootMabvuto BandaÎncă nu există evaluări
- Acute Lymphoblastic Leukemia - Ontologies - LabDocument6 paginiAcute Lymphoblastic Leukemia - Ontologies - LabAnusha SaiÎncă nu există evaluări
- Diabetic Foot Ulcer ReviewDocument7 paginiDiabetic Foot Ulcer Reviewintan_ekleÎncă nu există evaluări
- Intravascular Coagulation) Akibat Racun Gigitan Ular: Penyebaran Gumpalan Dalam Pembuluh Darah (DisseminatedDocument5 paginiIntravascular Coagulation) Akibat Racun Gigitan Ular: Penyebaran Gumpalan Dalam Pembuluh Darah (DisseminatedFenty SuwidakÎncă nu există evaluări
- A Review of The Pathophysiology, Classification, and Treatment of Foot Ulcers in Diabetic PatientsDocument7 paginiA Review of The Pathophysiology, Classification, and Treatment of Foot Ulcers in Diabetic Patientsmonikacholuj438Încă nu există evaluări
- A2 Group 3 GOUTDocument83 paginiA2 Group 3 GOUTArt Buenaventura0% (1)
- CaseDocument3 paginiCasesemajÎncă nu există evaluări
- Diabetic Foot Care GuideDocument28 paginiDiabetic Foot Care GuidePraneetha NouduriÎncă nu există evaluări
- Pendsey (2010) - Understanding Diabetic FootDocument6 paginiPendsey (2010) - Understanding Diabetic FootxtraqrkyÎncă nu există evaluări
- C PPPP "P P PP# PDocument11 paginiC PPPP "P P PP# PLeni CarununganÎncă nu există evaluări
- Jurnal ReadingDocument21 paginiJurnal ReadingWb Iqbal Tendi AlamÎncă nu există evaluări
- BIOCHEMICAL OF MUSCULOSKELETAL DISORDERDocument17 paginiBIOCHEMICAL OF MUSCULOSKELETAL DISORDERSyifa SalsabilaÎncă nu există evaluări
- The Diabetic Foot: Charcot Joint and Osteomyelitis: Laura Giurato and Luigi UccioliDocument5 paginiThe Diabetic Foot: Charcot Joint and Osteomyelitis: Laura Giurato and Luigi UccioliRobert DwitamaÎncă nu există evaluări
- Kaki DiabetikDocument82 paginiKaki DiabetikNanda ValeriadiÎncă nu există evaluări
- Narrative PathophysiologyDocument4 paginiNarrative PathophysiologyChristine AlvarezÎncă nu există evaluări
- The Association Between Skin Blood Flow and Edema On Epidermal Thickness in The Diabetic FootDocument8 paginiThe Association Between Skin Blood Flow and Edema On Epidermal Thickness in The Diabetic FootdeborapkphnÎncă nu există evaluări
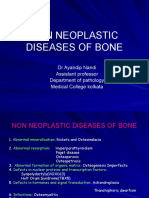
- Non-Neoplastic Bone Disease GuideDocument45 paginiNon-Neoplastic Bone Disease GuideKÎncă nu există evaluări
- OsteoarthritisDocument2 paginiOsteoarthritisDwipratiwi 2003Încă nu există evaluări
- K4 Matriks Ekstraseluler-20 PDFDocument46 paginiK4 Matriks Ekstraseluler-20 PDFnaysonÎncă nu există evaluări
- Diseases of Bone: Brig Shahid Jamal MBBS, Fcps (Pak), Frcpath (Uk) Professor of Histopathology Am College RawalpindiDocument27 paginiDiseases of Bone: Brig Shahid Jamal MBBS, Fcps (Pak), Frcpath (Uk) Professor of Histopathology Am College RawalpindiMuhammad IqbalÎncă nu există evaluări
- Diabetic Foot Disease: Rizki Yaruntradhani Pradwipa MD, B. Med. SCDocument37 paginiDiabetic Foot Disease: Rizki Yaruntradhani Pradwipa MD, B. Med. SCRacheal KellyÎncă nu există evaluări
- Patient Education: Preventing Diabetic Foot InfectionsDocument9 paginiPatient Education: Preventing Diabetic Foot InfectionsBrîndușa PetruțescuÎncă nu există evaluări
- Metabolic Bone DiseaseDocument25 paginiMetabolic Bone DiseaseSavin PetersÎncă nu există evaluări
- Charcot MarkDocument52 paginiCharcot MarkIgnacio ToledoÎncă nu există evaluări
- 18 Diseases of The Joints 1 - 2021Document46 pagini18 Diseases of The Joints 1 - 2021Ahmed YTÎncă nu există evaluări
- Rhabdomyolysis - PACTDocument2 paginiRhabdomyolysis - PACTSanj.etcÎncă nu există evaluări
- JointsDocument68 paginiJointsLaine ZeeÎncă nu există evaluări
- Orthopedicdisorders 121221093512 Phpapp01Document93 paginiOrthopedicdisorders 121221093512 Phpapp01sarikaÎncă nu există evaluări
- Diabetes and Its Effect On Wound Healing 20910Document12 paginiDiabetes and Its Effect On Wound Healing 20910DesyPratiwiWidjajanaÎncă nu există evaluări
- Multiple MyelomaDocument20 paginiMultiple Myelomaasim badarÎncă nu există evaluări
- The Diabetic FootDocument12 paginiThe Diabetic FootOliver Vebrian SampelilingÎncă nu există evaluări
- Diabetic Foot Pathophysiology and Risk FactorsDocument8 paginiDiabetic Foot Pathophysiology and Risk FactorsKat BausaÎncă nu există evaluări
- Agis Mira Dewi, S.kedDocument35 paginiAgis Mira Dewi, S.kedAgiish EMdeÎncă nu există evaluări
- Diabetes - Mellitus 16 12 14Document25 paginiDiabetes - Mellitus 16 12 14David NicholasÎncă nu există evaluări
- Crystal Deposition Disorders ReviewDocument68 paginiCrystal Deposition Disorders ReviewMustafa Abbas AlObaidyÎncă nu există evaluări
- Imaging Techniques for Diabetic Foot ComplicationsDocument10 paginiImaging Techniques for Diabetic Foot ComplicationsEka JuliantaraÎncă nu există evaluări
- OSTEOARTHRITISDocument29 paginiOSTEOARTHRITISValabhoju Bindu MadhaviÎncă nu există evaluări
- Asam UratDocument43 paginiAsam UratIhsan AndanÎncă nu există evaluări
- Komplikasi Diabetes 2015Document55 paginiKomplikasi Diabetes 2015AchmadRizaÎncă nu există evaluări
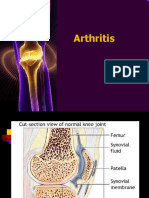
- Arthritis 180325095830 PDFDocument77 paginiArthritis 180325095830 PDFHesoca HuxÎncă nu există evaluări
- Diabetic FootDocument188 paginiDiabetic FootSushil VijayÎncă nu există evaluări
- Bone andDocument33 paginiBone andSuci MayveraÎncă nu există evaluări
- Diabetic Foot Ulcer - Yandriyane Stephanie Robiady - 131621190504Document28 paginiDiabetic Foot Ulcer - Yandriyane Stephanie Robiady - 131621190504Yohelio Priawan SibuÎncă nu există evaluări
- OsteoarthritisDocument25 paginiOsteoarthritisRaymund Christopher Dela PeñaÎncă nu există evaluări
- Hev Easl CPGDocument45 paginiHev Easl CPGRaluca-Elena AlexaÎncă nu există evaluări
- Manual CBC 1 3: - Wbcs - Platelets Count - PCV or HCT - Retics Count - HB Estimation 3 3 4 5 6Document25 paginiManual CBC 1 3: - Wbcs - Platelets Count - PCV or HCT - Retics Count - HB Estimation 3 3 4 5 6Aqila MumtazÎncă nu există evaluări
- 4.5. How To Test - Testing Strategy HBV Decision-Making Tables - PICO 3Document10 pagini4.5. How To Test - Testing Strategy HBV Decision-Making Tables - PICO 3Aqila MumtazÎncă nu există evaluări
- Bdb06ff135c7ccb File 2Document29 paginiBdb06ff135c7ccb File 2Mary ThaherÎncă nu există evaluări
- Lung CaDocument1 paginăLung CaAqila MumtazÎncă nu există evaluări
- Weight Percentiles CalculatorDocument1 paginăWeight Percentiles CalculatorAqila MumtazÎncă nu există evaluări
- Study Guide Public Health Chapter 6Document2 paginiStudy Guide Public Health Chapter 6Aqila MumtazÎncă nu există evaluări
- BST Notes GRRRRDocument5 paginiBST Notes GRRRRAqila MumtazÎncă nu există evaluări
- Clinical Practice Guidelines for Hepatitis B Virus (HBV) ManagementDocument48 paginiClinical Practice Guidelines for Hepatitis B Virus (HBV) ManagementAqila MumtazÎncă nu există evaluări
- Assessing Dehydration Chart Msword 485697997Document2 paginiAssessing Dehydration Chart Msword 485697997Aqila MumtazÎncă nu există evaluări
- Approach of TraumaDocument45 paginiApproach of TraumaAqila MumtazÎncă nu există evaluări
- Palsnewpacket PDFDocument29 paginiPalsnewpacket PDFAqila MumtazÎncă nu există evaluări
- Assignments 2016: M T W T F S SDocument12 paginiAssignments 2016: M T W T F S SAqila MumtazÎncă nu există evaluări
- Weight Percentiles CalculatorDocument1 paginăWeight Percentiles CalculatorAqila MumtazÎncă nu există evaluări
- DKA Study GroupDocument24 paginiDKA Study GroupAqila MumtazÎncă nu există evaluări
- BirdbrainDocument1 paginăBirdbrainplastoneÎncă nu există evaluări
- Dengue Fever TutorialDocument3 paginiDengue Fever TutorialAqila MumtazÎncă nu există evaluări
- Traumatic Brain Injury LectureDocument12 paginiTraumatic Brain Injury LectureAqila MumtazÎncă nu există evaluări
- Hyperglycemic Hyperosmolar StateDocument17 paginiHyperglycemic Hyperosmolar StateAqila Mumtaz50% (2)
- ParkinsonDocument5 paginiParkinsonAqila MumtazÎncă nu există evaluări
- BED SITE NOTE - Guillain Barre SyndromeDocument2 paginiBED SITE NOTE - Guillain Barre SyndromeAqila MumtazÎncă nu există evaluări
- Ethics Approval2013 - NewDocument8 paginiEthics Approval2013 - NewAqila MumtazÎncă nu există evaluări
- Treatment and Management of AstrocytomaDocument2 paginiTreatment and Management of AstrocytomaAqila MumtazÎncă nu există evaluări
- Psychiatry MnemonicsDocument7 paginiPsychiatry MnemonicsFahad Almalki93% (15)
- Psychiatry MnemonicsDocument7 paginiPsychiatry MnemonicsFahad Almalki93% (15)
- Assignments 2016: M T W T F S SDocument12 paginiAssignments 2016: M T W T F S SAqila MumtazÎncă nu există evaluări
- Ac LeukemiaDocument10 paginiAc LeukemiaAqila MumtazÎncă nu există evaluări
- Dengue and Other Viral Hemorrhagic FeverDocument6 paginiDengue and Other Viral Hemorrhagic FeverAqila MumtazÎncă nu există evaluări
- HO OnG NotesDocument38 paginiHO OnG NotesAqila MumtazÎncă nu există evaluări
- Sop Standard Operating ProceduresDocument3 paginiSop Standard Operating ProceduresTaha SaadanÎncă nu există evaluări
- Institute for Biodiversity Research EstablishedDocument7 paginiInstitute for Biodiversity Research Establishedshami mohammedÎncă nu există evaluări
- Lantern October 2012Document36 paginiLantern October 2012Jovel JosephÎncă nu există evaluări
- Delivering Leftover Bread to Singapore's NeedyDocument14 paginiDelivering Leftover Bread to Singapore's Needywisemaverick_5084303Încă nu există evaluări
- Astm B805Document7 paginiAstm B805Jonicus-DextoreÎncă nu există evaluări
- Lec5. Classification of OrganismsDocument85 paginiLec5. Classification of OrganismsJohn Lawrence YbanezÎncă nu există evaluări
- How Your Personality Changes As You AgeDocument5 paginiHow Your Personality Changes As You AgeJulia BuslaevaÎncă nu există evaluări
- B&S - Immunoassay Market - Global Forecast To 2026Document36 paginiB&S - Immunoassay Market - Global Forecast To 2026VK KRISHNAMOORTHYÎncă nu există evaluări
- Business Permits and Licensing Office/ Lgu-Tubigon, BoholDocument20 paginiBusiness Permits and Licensing Office/ Lgu-Tubigon, BoholMARILOU DAGUIOÎncă nu există evaluări
- Tracking Our Progress: Leverage Our Win in The UNIQUE 24/7 Marketplace PortfolioDocument8 paginiTracking Our Progress: Leverage Our Win in The UNIQUE 24/7 Marketplace PortfolioMihaiÎncă nu există evaluări
- Activities For FinalsDocument10 paginiActivities For FinalsAmbita CherylÎncă nu există evaluări
- Preparing Equipment CalibrationDocument1 paginăPreparing Equipment CalibrationGlobal QualityÎncă nu există evaluări
- Fluke 187 - 189 Manual de CalibracionDocument38 paginiFluke 187 - 189 Manual de Calibracionflavio torresÎncă nu există evaluări
- 10 1016@j Psep 2020 05 034Document82 pagini10 1016@j Psep 2020 05 034Kevin SalvatierraÎncă nu există evaluări
- PGN - ITP Dan Typical Drawing MRS 2020 Untuk Referensi Quotation 2020Document35 paginiPGN - ITP Dan Typical Drawing MRS 2020 Untuk Referensi Quotation 2020adjiÎncă nu există evaluări
- Final Study SS of 2nd PB 2023Document65 paginiFinal Study SS of 2nd PB 2023rahul SÎncă nu există evaluări
- Prepare Starch DishesDocument31 paginiPrepare Starch DishesAel Baguisi71% (7)
- Abdulrahman 4 Bashir Abdirahman Hussein STR .BPNDocument1 paginăAbdulrahman 4 Bashir Abdirahman Hussein STR .BPNFrancis OdongoÎncă nu există evaluări
- ACHE Fin Fan TechDocument15 paginiACHE Fin Fan TechAnonymous 8Mc8boONÎncă nu există evaluări
- การเคลื่อนที่ของสิ่งมีชีวิตDocument1 paginăการเคลื่อนที่ของสิ่งมีชีวิตธีรนัย เสารางทอยÎncă nu există evaluări
- gk1630t, 1640t - GB - md09Document16 paginigk1630t, 1640t - GB - md09Anonymous Y64YEIlÎncă nu există evaluări
- Digital biometric ruler for eye measurementsDocument2 paginiDigital biometric ruler for eye measurementsFrancisco GomezÎncă nu există evaluări
- People V Veneracion Case DigestDocument3 paginiPeople V Veneracion Case DigestraykarloBÎncă nu există evaluări
- Electric Vehicle Safety SheetDocument2 paginiElectric Vehicle Safety SheetRob NikolewskiÎncă nu există evaluări
- Effects of Parental Separation and DivorceDocument3 paginiEffects of Parental Separation and DivorceJoy PascoÎncă nu există evaluări
- RD ChecklistDocument14 paginiRD Checklistwerismy daddyÎncă nu există evaluări
- WP104 PDFDocument33 paginiWP104 PDFDiah wuri andaniÎncă nu există evaluări
- RVLineDocument28 paginiRVLinesghscribd2012Încă nu există evaluări
- Climate Factsheets July 2022Document7 paginiClimate Factsheets July 2022Michael SiaÎncă nu există evaluări
- IGA Report FINAL 10 07 2016Document171 paginiIGA Report FINAL 10 07 2016Timothy SchwartzÎncă nu există evaluări