S-ar putea să vă placă și
- Ministry of Health Price List For Ambulatory and Hospitalization ServicesDocument40 paginiMinistry of Health Price List For Ambulatory and Hospitalization ServicesHåíthãm KhãtïßÎncă nu există evaluări
- Ministry of Health Price List For Ambulatory and Hospitalization ServicesDocument49 paginiMinistry of Health Price List For Ambulatory and Hospitalization ServicesHåíthãm KhãtïßÎncă nu există evaluări
- YY תרגול כיתתי- גדילה, תזונה ומטבוליזם PDFDocument125 paginiYY תרגול כיתתי- גדילה, תזונה ומטבוליזם PDFHåíthãm KhãtïßÎncă nu există evaluări
- Zarif Qaraqra English Section, Seria A, 6 Group 1, 2020 - 2021Document3 paginiZarif Qaraqra English Section, Seria A, 6 Group 1, 2020 - 2021Håíthãm KhãtïßÎncă nu există evaluări
- Surgery 2 PDFDocument176 paginiSurgery 2 PDFHåíthãm KhãtïßÎncă nu există evaluări
- Surgery 3 White Part 1Document87 paginiSurgery 3 White Part 1Håíthãm KhãtïßÎncă nu există evaluări
- Surgery 1 PDFDocument183 paginiSurgery 1 PDFHåíthãm KhãtïßÎncă nu există evaluări
- Goal:: Practical Activity in Clinic (Oncalls)Document60 paginiGoal:: Practical Activity in Clinic (Oncalls)Håíthãm KhãtïßÎncă nu există evaluări
- Breast Slide DeckDocument34 paginiBreast Slide DeckJane ViÎncă nu există evaluări
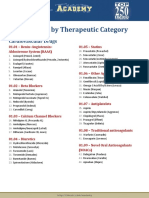
- Drug List by Therapeutic Category: Cardiovascular DrugsDocument7 paginiDrug List by Therapeutic Category: Cardiovascular DrugsAloah122346Încă nu există evaluări
- Hepatitis A VaccineDocument5 paginiHepatitis A VaccineHåíthãm KhãtïßÎncă nu există evaluări
- Hepatitis B Vaccine: Dosage Forms & StrengthsDocument3 paginiHepatitis B Vaccine: Dosage Forms & StrengthsHåíthãm KhãtïßÎncă nu există evaluări
- 3 Tier Drug List: CaliforniaDocument154 pagini3 Tier Drug List: CaliforniaHåíthãm KhãtïßÎncă nu există evaluări
- Neisseria Genus EnglDocument127 paginiNeisseria Genus EnglHåíthãm KhãtïßÎncă nu există evaluări
- Abc of Drug 1Document130 paginiAbc of Drug 1Håíthãm KhãtïßÎncă nu există evaluări
- Curs Epitelii EnglezaDocument50 paginiCurs Epitelii EnglezaHåíthãm KhãtïßÎncă nu există evaluări
- Genetic DiseasesDocument43 paginiGenetic DiseasesAisha BirdÎncă nu există evaluări
- Connective Tissue HistologyDocument12 paginiConnective Tissue HistologyHåíthãm KhãtïßÎncă nu există evaluări
- Corynebacterium Listeria EnlgDocument97 paginiCorynebacterium Listeria EnlgHåíthãm KhãtïßÎncă nu există evaluări
- Genetic DiseasesDocument43 paginiGenetic DiseasesAisha BirdÎncă nu există evaluări
- Immune System Has Two Lines of Defense:: A. Innate (Non Specific) ImmunityDocument105 paginiImmune System Has Two Lines of Defense:: A. Innate (Non Specific) ImmunityHåíthãm KhãtïßÎncă nu există evaluări
- Curs 3 Lecture Nutrition and Bacteria CultivationDocument74 paginiCurs 3 Lecture Nutrition and Bacteria CultivationHåíthãm KhãtïßÎncă nu există evaluări
- 5 DR Farhat MoazamDocument9 pagini5 DR Farhat MoazamHåíthãm KhãtïßÎncă nu există evaluări
- Curs 1 - 2 EnglDocument213 paginiCurs 1 - 2 EnglHåíthãm KhãtïßÎncă nu există evaluări
- Automated External Defibrillation - A0Document1 paginăAutomated External Defibrillation - A0Håíthãm KhãtïßÎncă nu există evaluări
- Breast CancerDocument53 paginiBreast Cancersmbala100% (1)
- Goal:: Practical Activity in Clinic (Oncalls)Document60 paginiGoal:: Practical Activity in Clinic (Oncalls)Håíthãm KhãtïßÎncă nu există evaluări
- Abiliti 2Document68 paginiAbiliti 2Håíthãm KhãtïßÎncă nu există evaluări
- VaksinasiDocument54 paginiVaksinasinikeÎncă nu există evaluări
- Breast CancerDocument52 paginiBreast CancerazharyekaputraÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Global Environment Unit 2Document13 paginiGlobal Environment Unit 2Se SathyaÎncă nu există evaluări
- Al Khudari Company Profile FP PDFDocument14 paginiAl Khudari Company Profile FP PDFAnonymous bgYdp4Încă nu există evaluări
- Sale of Property When - KP AstrologyDocument2 paginiSale of Property When - KP Astrologyprajishvet100% (1)
- Uptime KitsDocument3 paginiUptime KitsMtto Materia PrimaÎncă nu există evaluări
- Rig 166 Data SheetDocument2 paginiRig 166 Data SheetEstuardo OlanÎncă nu există evaluări
- Astro 429 Assignment 2 AlbertaDocument2 paginiAstro 429 Assignment 2 AlbertatarakÎncă nu există evaluări
- Form 03B Heritage Bell 1Document2 paginiForm 03B Heritage Bell 1ValÎncă nu există evaluări
- kAmAxI Muka Panchashati EngDocument25 paginikAmAxI Muka Panchashati EngSrinathvr100% (1)
- Chapter 01 Vacuum Chambers Special Components PDFDocument14 paginiChapter 01 Vacuum Chambers Special Components PDFmindrumihaiÎncă nu există evaluări
- Remote Control Based Home Appliances Final ReportDocument22 paginiRemote Control Based Home Appliances Final ReportVishal Vn50% (2)
- Journal of Environmental Management: Ajay Singh TDocument7 paginiJournal of Environmental Management: Ajay Singh TNestor Garay CahuanaÎncă nu există evaluări
- StringTokenizer in JavaDocument11 paginiStringTokenizer in JavaNeha saxena Neha saxenaÎncă nu există evaluări
- En 13757 3 2018 04Document104 paginiEn 13757 3 2018 04Hélder Vieira100% (1)
- IJHIM 6 - Nur Husnina (36 SD 42)Document7 paginiIJHIM 6 - Nur Husnina (36 SD 42)RSU Sayang BundaÎncă nu există evaluări
- Hemodynamic Monitoring in ICUDocument111 paginiHemodynamic Monitoring in ICUManjunath Gemini100% (2)
- TMJDocument38 paginiTMJAnonymous 6kAmeZzIÎncă nu există evaluări
- Details of Placed Students in Academic Session 2022-23Document10 paginiDetails of Placed Students in Academic Session 2022-23Rahul MishraÎncă nu există evaluări
- Method Statement of T-Beams PDFDocument14 paginiMethod Statement of T-Beams PDFKAmi KaMranÎncă nu există evaluări
- Jason Read, "Real Subsumption"Document32 paginiJason Read, "Real Subsumption"Aren Z. AizuraÎncă nu există evaluări
- Gas Permeability, Diffusivity and Solubility of Nitrogen, Helium, Methane, CO2, CH2O in Dense Polymeric Membranes Using A New On-Line Permeation ApparatusDocument12 paginiGas Permeability, Diffusivity and Solubility of Nitrogen, Helium, Methane, CO2, CH2O in Dense Polymeric Membranes Using A New On-Line Permeation ApparatusCinthiaCevallosÎncă nu există evaluări
- 1 N117Geriatric Nursing Lecture 1 BABY BOOMERSDocument4 pagini1 N117Geriatric Nursing Lecture 1 BABY BOOMERSqygwfvbysgbcnntgrvbÎncă nu există evaluări
- Ags 30Document1 paginăAgs 30Anonymous jIzz7woS60% (1)
- Daily Lesson Log 4Document5 paginiDaily Lesson Log 4Diane Marr Nicolas Dencio100% (2)
- HISTOPATHDocument38 paginiHISTOPATHDennis Louis Montepio BrazaÎncă nu există evaluări
- Kids and Their Favourite Food Key Reading Comprehension Exercises - 34436Document2 paginiKids and Their Favourite Food Key Reading Comprehension Exercises - 34436MonicaMartirosyanÎncă nu există evaluări
- MHFU Hunter RankDocument5 paginiMHFU Hunter RankGustin PrayogoÎncă nu există evaluări
- Carcass Strength Relationships Conveyor BeltsDocument9 paginiCarcass Strength Relationships Conveyor Beltseduardo_chaban100% (1)
- Optimizing With eGaN FETsDocument6 paginiOptimizing With eGaN FETskhsniperÎncă nu există evaluări
- Part PabrikDocument2 paginiPart PabrikNaldy NaldyÎncă nu există evaluări
- Compressed Air Pressure Drop DiagramDocument4 paginiCompressed Air Pressure Drop DiagramycemalÎncă nu există evaluări