S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- Mobilization NotesDocument239 paginiMobilization NotesSuganya Balachandran100% (6)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Biology PDFDocument1.447 paginiBiology PDFPrincess Ethel Atillo100% (2)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- How Can We Use Neurotransmitters in Emotion and Reward System To Study DepressionDocument22 paginiHow Can We Use Neurotransmitters in Emotion and Reward System To Study DepressionGlobal Research and Development ServicesÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Essential Ayurveda BookDocument196 paginiEssential Ayurveda BookRoberto89% (9)
- What Are The Types of EndosDocument3 paginiWhat Are The Types of EndosSailu KatragaddaÎncă nu există evaluări
- Nursing Care Plan for CVA Bleeding PatientDocument3 paginiNursing Care Plan for CVA Bleeding PatientpaulaÎncă nu există evaluări
- L.D..Occlusion in FPDDocument138 paginiL.D..Occlusion in FPDApurva Deshmukh67% (3)
- Answer Key For Comprehensive Exam XVDocument18 paginiAnswer Key For Comprehensive Exam XVQharts SajiranÎncă nu există evaluări
- NTSE Stage 1 State Level Model Paper 14Document4 paginiNTSE Stage 1 State Level Model Paper 14AmanÎncă nu există evaluări
- Chronobiology and Anesthesia: Review ArticleDocument15 paginiChronobiology and Anesthesia: Review ArticleGabriela Lizbeth ArmentaÎncă nu există evaluări
- Pancoast Tumour: Rare Lung Cancer FormDocument2 paginiPancoast Tumour: Rare Lung Cancer FormobligatraftelÎncă nu există evaluări
- Anatomy 2ND de BachilleratoDocument24 paginiAnatomy 2ND de BachilleratoAlexander IntriagoÎncă nu există evaluări
- Nervous System - All NotesDocument6 paginiNervous System - All NotesJÎncă nu există evaluări
- Supranuclear Control Opf Eye MovementsDocument162 paginiSupranuclear Control Opf Eye Movementsknowledgeguruos179Încă nu există evaluări
- Zoology: Zoology Previous Eamcet QuestionsDocument8 paginiZoology: Zoology Previous Eamcet QuestionsGaganpreetSingh100% (1)
- 2018 Life Sciences Tsset (Answers With Explanation)Document24 pagini2018 Life Sciences Tsset (Answers With Explanation)Swetha SrigirirajuÎncă nu există evaluări
- Circulatory System: Heart, Blood Vessels & Their FunctionsDocument17 paginiCirculatory System: Heart, Blood Vessels & Their FunctionskangaanushkaÎncă nu există evaluări
- Tetralogy of Fallot Everything You Wanted To Know But Were Afraid To AskDocument8 paginiTetralogy of Fallot Everything You Wanted To Know But Were Afraid To AsksofiaÎncă nu există evaluări
- GIT Physio D&R AgamDocument67 paginiGIT Physio D&R Agamvisweswar030406Încă nu există evaluări
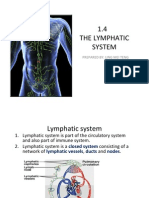
- 1.4 The Lymphatic System: Prepared By: Ling Mei TengDocument15 pagini1.4 The Lymphatic System: Prepared By: Ling Mei TengJuliet LingÎncă nu există evaluări
- Identification of BacteriaDocument4 paginiIdentification of BacteriaVasugiÎncă nu există evaluări
- Anatomy and Physiology-REVIEWER-Practical ExamDocument12 paginiAnatomy and Physiology-REVIEWER-Practical ExamDeity Ann ReuterezÎncă nu există evaluări
- Worksheet: I) Ii) Iii)Document4 paginiWorksheet: I) Ii) Iii)Jin MingÎncă nu există evaluări
- The Anterior Cranial FossaDocument4 paginiThe Anterior Cranial FossaArshad hussainÎncă nu există evaluări
- ANAESTHESIOLOGYDocument38 paginiANAESTHESIOLOGYcollinsmagÎncă nu există evaluări
- January 2016 (IAL) QP - Unit 1 Edexcel Biology A-LevelDocument24 paginiJanuary 2016 (IAL) QP - Unit 1 Edexcel Biology A-LevelkirthikaÎncă nu există evaluări
- Journal Reading Radiologi EllaDocument44 paginiJournal Reading Radiologi EllaElla Putri SaptariÎncă nu există evaluări
- Altitude PhysiologyDocument41 paginiAltitude Physiologyshepherd jeremiahÎncă nu există evaluări
- Super 108 DR LalDocument8 paginiSuper 108 DR Lalarkaprava paulÎncă nu există evaluări
- CM All Compiled NotesDocument100 paginiCM All Compiled NotesKatrina Mae PatalinghugÎncă nu există evaluări