S-ar putea să vă placă și
- 10Document3 pagini10Rivan San JayaÎncă nu există evaluări
- Artikan 3Document1 paginăArtikan 3Rivan San JayaÎncă nu există evaluări
- Jay A. PermanDocument40 paginiJay A. PermanRivan San JayaÎncă nu există evaluări
- 5.impact of Obesity On Gynecology - Shilpi Pandey, Siladitya Bhattacharya, 2010Document26 pagini5.impact of Obesity On Gynecology - Shilpi Pandey, Siladitya Bhattacharya, 2010Rivan San JayaÎncă nu există evaluări
- RNC Kendari1 Native IP Datafill V19.0 - 10 Nov 2015Document234 paginiRNC Kendari1 Native IP Datafill V19.0 - 10 Nov 2015Rivan San JayaÎncă nu există evaluări
- Maintenance Visit ReportDocument5 paginiMaintenance Visit ReportRivan San JayaÎncă nu există evaluări
- January - Hirschsprung's Disease in Africa 21 CenturyDocument27 paginiJanuary - Hirschsprung's Disease in Africa 21 CenturyVita MadmoÎncă nu există evaluări
- RNC Kendari1 Native IP Datafill V19.0 - 10 Nov 2015Document234 paginiRNC Kendari1 Native IP Datafill V19.0 - 10 Nov 2015Rivan San JayaÎncă nu există evaluări
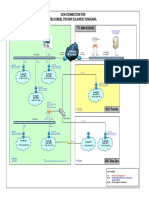
- Visio-121123 DCN Drawing For PC-MG PDH Sultengra (General)Document1 paginăVisio-121123 DCN Drawing For PC-MG PDH Sultengra (General)Rivan San JayaÎncă nu există evaluări
- Site List Delay - Sumalirja - Part-1Document14 paginiSite List Delay - Sumalirja - Part-1Rivan San JayaÎncă nu există evaluări
- RNCN - KDI2 Native IP Datafill V8 9 - 23 Okt 2015Document106 paginiRNCN - KDI2 Native IP Datafill V8 9 - 23 Okt 2015Rivan San JayaÎncă nu există evaluări
- Site List Delay - Sumalirja - Part-1Document14 paginiSite List Delay - Sumalirja - Part-1Rivan San JayaÎncă nu există evaluări
- Ping MSC KendariDocument6 paginiPing MSC KendariRivan San JayaÎncă nu există evaluări
- Monitoring Nec KendariDocument4 paginiMonitoring Nec KendariRivan San JayaÎncă nu există evaluări
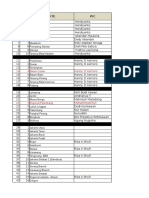
- Inventaris ITDocument1 paginăInventaris ITRivan San JayaÎncă nu există evaluări
- Ping NMS PDH Kendari To Server MakasarDocument3 paginiPing NMS PDH Kendari To Server MakasarRivan San JayaÎncă nu există evaluări
- Lamar AnDocument6 paginiLamar AnRivan San JayaÎncă nu există evaluări
- Schedule Implementation IP Management - v11Document10 paginiSchedule Implementation IP Management - v11Rivan San JayaÎncă nu există evaluări
- Img 20151102 0028Document1 paginăImg 20151102 0028Rivan San JayaÎncă nu există evaluări
- Setting OutlookDocument2 paginiSetting OutlookRivan San JayaÎncă nu există evaluări
- Img 20151107 0021Document1 paginăImg 20151107 0021Rivan San JayaÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Vestigial Organs 1Document3 paginiVestigial Organs 1api-711119679Încă nu există evaluări
- Research Titles From 2005 To 2022Document490 paginiResearch Titles From 2005 To 2022AMOLÎncă nu există evaluări
- Informatics Activity 3Document39 paginiInformatics Activity 3Jouella AnneÎncă nu există evaluări
- Timing of Antimicrobial Prophylaxis and Infectious Complications in Pediatric Patients Undergoing AppendicectomyDocument3 paginiTiming of Antimicrobial Prophylaxis and Infectious Complications in Pediatric Patients Undergoing AppendicectomyJuan J. Acosta VelásquezÎncă nu există evaluări
- Artikel Yang Telah Terakreditasi HONcodeDocument5 paginiArtikel Yang Telah Terakreditasi HONcoderidhola15Încă nu există evaluări
- The Surgical Examination of ChildrenDocument315 paginiThe Surgical Examination of ChildrencutlisaafriannaÎncă nu există evaluări
- AppendicitisDocument14 paginiAppendicitispreethijojo2003558288% (8)
- Thesis Medical Surgical NursingDocument5 paginiThesis Medical Surgical Nursingafbsbwceg100% (1)
- Dr. Zaka Ur Rab Siddiqui - Senior Surgeon Laparoscopic-Bariatric Frcs-Fcps-MrcsDocument5 paginiDr. Zaka Ur Rab Siddiqui - Senior Surgeon Laparoscopic-Bariatric Frcs-Fcps-MrcscdeekyÎncă nu există evaluări
- AMC Anthology of Medical Conditions - UnlockedDocument483 paginiAMC Anthology of Medical Conditions - UnlockedSherif Elbadrawy92% (12)
- Surgical Nursing McQsDocument10 paginiSurgical Nursing McQsAmisalu NigusieÎncă nu există evaluări
- Castor Oil Pack Ebook PDFDocument22 paginiCastor Oil Pack Ebook PDFKenneth Woo100% (8)
- Acute Abdomen: The "Black Hole" of MedicineDocument97 paginiAcute Abdomen: The "Black Hole" of Medicineedward iskandarÎncă nu există evaluări
- Daftar Pustaka - RioDocument4 paginiDaftar Pustaka - RioRyo ChairulÎncă nu există evaluări
- Surgery PackratDocument46 paginiSurgery PackratRicardo Nelson100% (4)
- Critical Appraisal KADocument35 paginiCritical Appraisal KAKentVilandkaÎncă nu există evaluări
- NCP AppendicitisDocument2 paginiNCP AppendicitisArnel Luces Beato100% (1)
- PMDC NEB Exam Medical FormatDocument6 paginiPMDC NEB Exam Medical FormatShawn Parker57% (7)
- Rincian Kewenangan Klinis AnakDocument6 paginiRincian Kewenangan Klinis AnakUchiha ItachiÎncă nu există evaluări
- AppendicitisDocument21 paginiAppendicitisathya100% (1)
- 2.1 Medical Surgical Nursing - I Papers QPDocument15 pagini2.1 Medical Surgical Nursing - I Papers QPAnju KarunakaranÎncă nu există evaluări
- Medical Surgical Nursing Exams BoardDocument36 paginiMedical Surgical Nursing Exams BoardCINDY� BELMESÎncă nu există evaluări
- Acute Appendicitis & NPI - Edmalyn GozarDocument78 paginiAcute Appendicitis & NPI - Edmalyn GozarKM100% (1)
- Matary Cases 2013Document153 paginiMatary Cases 2013Raouf Ra'fat Soliman100% (10)
- Abdominal PainDocument16 paginiAbdominal PainSumit KhetarpalÎncă nu există evaluări
- Case 2 H PDocument3 paginiCase 2 H Papi-356483382100% (1)
- Diseases of Digestive SystemDocument87 paginiDiseases of Digestive SystemEdgar Jr. CustodioÎncă nu există evaluări
- 3 AnaesDocument9 pagini3 Anaessiti israwatiÎncă nu există evaluări
- Emergencies in GITDocument7 paginiEmergencies in GITsssajiÎncă nu există evaluări
- Anterior Abdominal WallDocument5 paginiAnterior Abdominal WallAnonymous 2TzM1ZÎncă nu există evaluări