S-ar putea să vă placă și
- Urgentcare FormDocument4 paginiUrgentcare Formapi-287654333Încă nu există evaluări
- PDF Staff Application07 2018Document3 paginiPDF Staff Application07 2018HummÎncă nu există evaluări
- Self Pay Information FormDocument1 paginăSelf Pay Information FormPerformax Physical TherapyÎncă nu există evaluări
- Memorial Hermann Discharge Papers - 3Document5 paginiMemorial Hermann Discharge Papers - 3Alaska JamesÎncă nu există evaluări
- Onfidential Data Form: T L O S CDocument8 paginiOnfidential Data Form: T L O S Cnatpal100% (1)
- Patient Registration Form 29Document8 paginiPatient Registration Form 29Cahayastore CahayastoreÎncă nu există evaluări
- Patient Registration Form 13Document4 paginiPatient Registration Form 13windawaty humolaÎncă nu există evaluări
- Personnel Information Sheet (New) PDFDocument5 paginiPersonnel Information Sheet (New) PDFLoo PeaÎncă nu există evaluări
- (2010) Handbook Strategy As PracticeDocument367 pagini(2010) Handbook Strategy As PracticeViniciusÎncă nu există evaluări
- Key-Club-Membership-Form 1Document4 paginiKey-Club-Membership-Form 1api-461627977Încă nu există evaluări
- Fathers Day Sunday School LessonDocument10 paginiFathers Day Sunday School LessonMamienske FransÎncă nu există evaluări
- Candidate Application Form V2 23 June 2015 Neo EltariDocument4 paginiCandidate Application Form V2 23 June 2015 Neo Eltarianita nahakÎncă nu există evaluări
- Discipline and Ideas QuestonaireDocument3 paginiDiscipline and Ideas QuestonaireShaira Mae Pasion Erdaje100% (1)
- Student Profile Form For Inventory - PDFDocument2 paginiStudent Profile Form For Inventory - PDFLeen Ganoran100% (1)
- Employment Application Form 09Document3 paginiEmployment Application Form 09api-19987040Încă nu există evaluări
- Adult Learning An OverviewDocument11 paginiAdult Learning An OverviewKhalif AziziÎncă nu există evaluări
- Client - Interview Intake Form - Family LawDocument18 paginiClient - Interview Intake Form - Family Lawgernsby935100% (1)
- Official Medical Information and Release FormDocument2 paginiOfficial Medical Information and Release FormtheNOLAtreeÎncă nu există evaluări
- History Form For AdultsDocument9 paginiHistory Form For AdultsFazal HaqueÎncă nu există evaluări
- Student Assurance Services, Inc. P.O. Box 196 STILLWATER, MN 55082-0196Document1 paginăStudent Assurance Services, Inc. P.O. Box 196 STILLWATER, MN 55082-0196Sharif M Mizanur RahmanÎncă nu există evaluări
- Client Intake Form: (Last) (First) (MI)Document20 paginiClient Intake Form: (Last) (First) (MI)Prabha Gupta0% (1)
- Application For Admission: Please Note: This Entire Form Is To Be Completed by The Applicant. Please Print ClearlyDocument3 paginiApplication For Admission: Please Note: This Entire Form Is To Be Completed by The Applicant. Please Print ClearlyJanuhu ZakaryÎncă nu există evaluări
- Dube Trade Port Application FormDocument7 paginiDube Trade Port Application FormNcediswaÎncă nu există evaluări
- Enrollment AppDocument10 paginiEnrollment Appapi-218391675Încă nu există evaluări
- Applicant Application FormDocument6 paginiApplicant Application FormJocelyn Joy ArcegaÎncă nu există evaluări
- Adult NP Ppwrork KCPGDocument16 paginiAdult NP Ppwrork KCPGMary GreerÎncă nu există evaluări
- Electronic CKK 2018 AIT ApplicationDocument5 paginiElectronic CKK 2018 AIT ApplicationAnonymous kMFSq9ayGÎncă nu există evaluări
- Johnny Q - Employment Application FormDocument3 paginiJohnny Q - Employment Application Formprettyboiricky54Încă nu există evaluări
- Adult Client Intake Forms2Document7 paginiAdult Client Intake Forms2api-310813184Încă nu există evaluări
- Referral LetterDocument3 paginiReferral LetterMa. Thea Diane BillonesÎncă nu există evaluări
- Client medical history and treatment detailsDocument3 paginiClient medical history and treatment detailsMa. Thea Diane BillonesÎncă nu există evaluări
- HRD Form 001 Employee Application Gen - Admin v.001Document3 paginiHRD Form 001 Employee Application Gen - Admin v.001DadangÎncă nu există evaluări
- Employment Application: Safe Sanctuaries For Youth, or Santuarios Seguros Published by Discipleship Resources.)Document5 paginiEmployment Application: Safe Sanctuaries For Youth, or Santuarios Seguros Published by Discipleship Resources.)tncircuitriderÎncă nu există evaluări
- Life School Input SheetDocument1 paginăLife School Input Sheetapi-3703184Încă nu există evaluări
- Plex App Form 2022Document4 paginiPlex App Form 2022wjdhnpj4ndÎncă nu există evaluări
- Liability Release and Parental Consent FormDocument3 paginiLiability Release and Parental Consent Formapi-28674765Încă nu există evaluări
- Juvenile Justice Corps 2010-2011 ApplicationDocument4 paginiJuvenile Justice Corps 2010-2011 ApplicationCHCMCblog4085Încă nu există evaluări
- Allen County Board of DD Student Emergency DataDocument2 paginiAllen County Board of DD Student Emergency Dataadhi eng lrtÎncă nu există evaluări
- Teen MedicalDocument1 paginăTeen MedicalJohn C StarkÎncă nu există evaluări
- Submit This Application To Your Church LeadershipDocument4 paginiSubmit This Application To Your Church LeadershiparobinwaÎncă nu există evaluări
- 2011 GAME Waiver FormDocument1 pagină2011 GAME Waiver FormBrian LaRueÎncă nu există evaluări
- TEMPLATE Medical Release WITHOUT Notary 1Document1 paginăTEMPLATE Medical Release WITHOUT Notary 1Peter WagnerÎncă nu există evaluări
- Northern Spa Franchise Application SummaryDocument5 paginiNorthern Spa Franchise Application SummaryJannel VelascoÎncă nu există evaluări
- Application Form Youth For Development and Global XchangeDocument4 paginiApplication Form Youth For Development and Global Xchangeapi-26153714Încă nu există evaluări
- New Patient Forms PacketDocument4 paginiNew Patient Forms PacketCarrboro Family MedicineÎncă nu există evaluări
- Resident Leadership Program App Packet - Nov2018Document6 paginiResident Leadership Program App Packet - Nov2018Subhasis RoyÎncă nu există evaluări
- Patient FormsDocument4 paginiPatient Formsapi-203989638Încă nu există evaluări
- AS Nursing Student Health FormDocument4 paginiAS Nursing Student Health FormJane PÎncă nu există evaluări
- Medical FormDocument1 paginăMedical Formapi-144496227Încă nu există evaluări
- Empapp 2016 BDocument5 paginiEmpapp 2016 Bapi-393899350Încă nu există evaluări
- Brain Train Is 2015Document2 paginiBrain Train Is 2015scribdlertooÎncă nu există evaluări
- Guardian Angels Application: Paste Photograph Here After AcceptanceDocument3 paginiGuardian Angels Application: Paste Photograph Here After AcceptanceMary Jill VasquezÎncă nu există evaluări
- FNU Counselling Services Intake FormDocument2 paginiFNU Counselling Services Intake FormShanjni malaÎncă nu există evaluări
- Application FormDocument5 paginiApplication Formapi-26153714Încă nu există evaluări
- Health Statement FormDocument1 paginăHealth Statement FormALT IkedaÎncă nu există evaluări
- Appletree NP Forms FillableDocument2 paginiAppletree NP Forms FillableFabian SvrÎncă nu există evaluări
- Phlebotomy Tech FormDocument4 paginiPhlebotomy Tech FormHawaiiHealthCareÎncă nu există evaluări
- Emp Application Revised Feb 2006Document4 paginiEmp Application Revised Feb 2006Rachel HensleyÎncă nu există evaluări
- London Kids Admn Form - CDRDocument4 paginiLondon Kids Admn Form - CDRDeeniyat ChanserpurÎncă nu există evaluări
- Gauteng Dept of Health Bursary Application FormDocument4 paginiGauteng Dept of Health Bursary Application FormLerato bunnyÎncă nu există evaluări
- Application Form: FSL, 18 Waldstock Road, London, SE28 8SF Section 1Document5 paginiApplication Form: FSL, 18 Waldstock Road, London, SE28 8SF Section 1Niaz KhanÎncă nu există evaluări
- Employment Application for Office AdministratorDocument5 paginiEmployment Application for Office AdministratorVivian StanleyÎncă nu există evaluări
- Progressive Health Care: Critical Health Care InformationDe la EverandProgressive Health Care: Critical Health Care InformationÎncă nu există evaluări
- Sweet Success: Knowledge and Quick-Skills in Thirty MinutesDe la EverandSweet Success: Knowledge and Quick-Skills in Thirty MinutesÎncă nu există evaluări
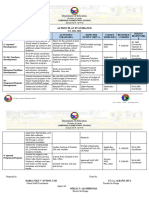
- ACTION PLAN IN GUIDANCE S.Y. 2021-2022Document2 paginiACTION PLAN IN GUIDANCE S.Y. 2021-2022Maria Noly Villotes EntinoÎncă nu există evaluări
- 9701 w13 QP 35 2 PDFDocument12 pagini9701 w13 QP 35 2 PDFNeural Spark Physics CieÎncă nu există evaluări
- To Study The Prevalence of Anaemia in Indoor Patients of Tertiary Care CentreDocument3 paginiTo Study The Prevalence of Anaemia in Indoor Patients of Tertiary Care CentreIJAR JOURNALÎncă nu există evaluări
- Talent Management in Malaysian UniversitDocument20 paginiTalent Management in Malaysian Universitحمب محمد نجمدنÎncă nu există evaluări
- Reg 20220716 Not WebpageDocument18 paginiReg 20220716 Not WebpageVandyÎncă nu există evaluări
- Cubeta Philosophy Managment LIBR204 081210bDocument18 paginiCubeta Philosophy Managment LIBR204 081210bjesscubesÎncă nu există evaluări
- Chem 105 Syllabus 2013 SpringDocument4 paginiChem 105 Syllabus 2013 SpringemuphychemÎncă nu există evaluări
- HDC CHÍNH THỨC TIẾNG ANH CHUYÊN 2022Document3 paginiHDC CHÍNH THỨC TIẾNG ANH CHUYÊN 2022Hoàng HuyÎncă nu există evaluări
- Using Historical Thinking to Teach GovernmentsDocument2 paginiUsing Historical Thinking to Teach GovernmentsSneha MishraÎncă nu există evaluări
- Proceedings LAMAS 5 2015 Edisi Revisi. Raheni Suhita, Djoko Sulaksono, Kenfitria Diah WDocument27 paginiProceedings LAMAS 5 2015 Edisi Revisi. Raheni Suhita, Djoko Sulaksono, Kenfitria Diah WAdam DamanhuriÎncă nu există evaluări
- Q1 LP AP WEEK 4 DAY 1-5Document5 paginiQ1 LP AP WEEK 4 DAY 1-5jessibel.alejandroÎncă nu există evaluări
- UNC Charlotte Magazine, 2Q, 2009Document46 paginiUNC Charlotte Magazine, 2Q, 2009unccharlotteÎncă nu există evaluări
- Family Breakdown PDFDocument11 paginiFamily Breakdown PDFSamantha GordonÎncă nu există evaluări
- Day 1 Introduction, Project Environment & Role of Project Manager (1) - Read-Only (53) - Read-OnlyDocument33 paginiDay 1 Introduction, Project Environment & Role of Project Manager (1) - Read-Only (53) - Read-OnlySuraj ShresthaÎncă nu există evaluări
- Intimate RelationshipDocument3 paginiIntimate RelationshipMelody LiuÎncă nu există evaluări
- Aliran SBP Tingkatan 4 Tahun 2015 & Laman Web Sekolah PDFDocument1 paginăAliran SBP Tingkatan 4 Tahun 2015 & Laman Web Sekolah PDFPaul Chan C LÎncă nu există evaluări
- Psychological Hardiness in Relation To Entrepreneurial Orientation Among Youth of PunjabDocument7 paginiPsychological Hardiness in Relation To Entrepreneurial Orientation Among Youth of PunjabPriyashree RoyÎncă nu există evaluări
- University of Southern Mindanao: Kabacan, Cotabato PhilippinesDocument7 paginiUniversity of Southern Mindanao: Kabacan, Cotabato PhilippinesAlexis banicioÎncă nu există evaluări
- Visualization Without VisionDocument21 paginiVisualization Without Vision11Dewi Meiliyan Ningrum dewimeiliyan.2020Încă nu există evaluări
- Weather Lesson PlanDocument13 paginiWeather Lesson Planapi-194520027Încă nu există evaluări
- Ebook PDF Theories of Personality 9th Edition by Jess Feist PDFDocument41 paginiEbook PDF Theories of Personality 9th Edition by Jess Feist PDFflossie.thompson26497% (29)
- USE OF ENGLISH REPORTED SPEECHDocument5 paginiUSE OF ENGLISH REPORTED SPEECHHuyền Phạm Thị NgọcÎncă nu există evaluări
- Theoretical FrameworkDocument3 paginiTheoretical FrameworkChristine GomezÎncă nu există evaluări
- Anallisis Lagu Lewis CapaldiDocument7 paginiAnallisis Lagu Lewis CapaldiIta PratiwiÎncă nu există evaluări
- Cs601pc - Machine Learning Unit - 2-1Document148 paginiCs601pc - Machine Learning Unit - 2-1RADHARAPU DIVYA PECÎncă nu există evaluări
- English 9 exam reading comprehension and language registersDocument5 paginiEnglish 9 exam reading comprehension and language registersAnjieyah Bersano FabroÎncă nu există evaluări