S-ar putea să vă placă și
- Clinical Research: Principles, Practice and PerspectiveDe la EverandClinical Research: Principles, Practice and PerspectiveÎncă nu există evaluări
- Clinical Section Coping Strategy Enhancement (CSE) : A Method of Treating Residual Schizophrenic SymptomsDocument11 paginiClinical Section Coping Strategy Enhancement (CSE) : A Method of Treating Residual Schizophrenic SymptomsSufira WahyuniÎncă nu există evaluări
- 2017-Ugo Chukwu-International Journal of Medicine and PharmacyDocument10 pagini2017-Ugo Chukwu-International Journal of Medicine and PharmacyNurettin AbacıoğluÎncă nu există evaluări
- Journal Presentation of Nisha LsDocument7 paginiJournal Presentation of Nisha LsANOOPVAÎncă nu există evaluări
- HHS Public Access: Medication Adherence Outcomes of 771 Intervention Trials: Systematic Review and Meta-AnalysisDocument21 paginiHHS Public Access: Medication Adherence Outcomes of 771 Intervention Trials: Systematic Review and Meta-Analysisdaniela NeculmanÎncă nu există evaluări
- Interventions in Nursing HomesDocument18 paginiInterventions in Nursing Homesvictory818Încă nu există evaluări
- Sedation Guidelines, Protocols, and Algorithms In.13Document8 paginiSedation Guidelines, Protocols, and Algorithms In.13Juan Pedro Alconada MaglianoÎncă nu există evaluări
- Manual Therapy: Neil Langridge, Lisa Roberts, Catherine PopeDocument6 paginiManual Therapy: Neil Langridge, Lisa Roberts, Catherine PopeVizaÎncă nu există evaluări
- 0146 6402 (94) 90001 9Document29 pagini0146 6402 (94) 90001 9sandra garcia molinaÎncă nu există evaluări
- 5-2016 42 Ijmah GoniometeryDocument7 pagini5-2016 42 Ijmah GoniometeryNatalie AcostaÎncă nu există evaluări
- What Is Missing From Descriptions of Treatment in Trials and Reviews?Document3 paginiWhat Is Missing From Descriptions of Treatment in Trials and Reviews?Fabricio LafebreÎncă nu există evaluări
- Patient CenteredDocument12 paginiPatient CenteredNina NaguyevskayaÎncă nu există evaluări
- The Effects of Pay-for-Performance Programs On Health, Health Care Use, and Processes of CareDocument14 paginiThe Effects of Pay-for-Performance Programs On Health, Health Care Use, and Processes of CareMasrun FatanahÎncă nu există evaluări
- Ebp Final DraftDocument14 paginiEbp Final Draftapi-436039292Încă nu există evaluări
- Out Come StudyDocument12 paginiOut Come StudyjaraÎncă nu există evaluări
- Eras Grand PDFDocument9 paginiEras Grand PDFWiwit ClimberÎncă nu există evaluări
- Schuffham - Using N-Of-1 Trials To Improve Patient Management and Save CostsDocument8 paginiSchuffham - Using N-Of-1 Trials To Improve Patient Management and Save CostsmitchxpÎncă nu există evaluări
- BMC Health Services ResearchDocument12 paginiBMC Health Services ResearchAgayatak Sa ManenÎncă nu există evaluări
- The Study of Drug Usage Patterns in Pediatric Patients at MGM Hospital, Navi MumbaiDocument10 paginiThe Study of Drug Usage Patterns in Pediatric Patients at MGM Hospital, Navi Mumbairajesh sumanÎncă nu există evaluări
- Evidence Based Practice FinalDocument22 paginiEvidence Based Practice Finalgopscharan100% (1)
- Paper Salud FamiliarDocument7 paginiPaper Salud FamiliarLucas Braga Almeida e SilvaÎncă nu există evaluări
- C P G: C C L B P: Riginal RticleDocument22 paginiC P G: C C L B P: Riginal RticleRajender BishtÎncă nu există evaluări
- Clinical Prediction Rules For Physical Therapy Interventions - A Systematic ReviewDocument13 paginiClinical Prediction Rules For Physical Therapy Interventions - A Systematic ReviewFilipe Mello MedeirosÎncă nu există evaluări
- Making Informed Decisions: Assessing Strengths and Weaknesses of Study Designs and Analytic Methods For Comparative Effectiveness ResearchDocument36 paginiMaking Informed Decisions: Assessing Strengths and Weaknesses of Study Designs and Analytic Methods For Comparative Effectiveness ResearchNational Pharmaceutical CouncilÎncă nu există evaluări
- The Need For Pharmaceutical Care in An Intensive Care Unit at A Teaching Hospital in South AfricaDocument4 paginiThe Need For Pharmaceutical Care in An Intensive Care Unit at A Teaching Hospital in South AfricaAdibaÎncă nu există evaluări
- Developing A Measure For The Appropriateness of Prescribing in General PracticeDocument5 paginiDeveloping A Measure For The Appropriateness of Prescribing in General Practiceujangketul62Încă nu există evaluări
- HLTH 520 Reseach Appraisal - ResearchDocument16 paginiHLTH 520 Reseach Appraisal - Researchapi-479186899Încă nu există evaluări
- Aresearch Investigationinto The Utilizationof Thepqrstnursingcarestrategy Amongnursing Pre-ProfessionalsDocument11 paginiAresearch Investigationinto The Utilizationof Thepqrstnursingcarestrategy Amongnursing Pre-ProfessionalsIJAR JOURNALÎncă nu există evaluări
- Perceptions of The Professional Pharmacy Services in A Major Canadian Hospital: A Comparison of Stakeholder GroupsDocument12 paginiPerceptions of The Professional Pharmacy Services in A Major Canadian Hospital: A Comparison of Stakeholder GroupsGracia GiasiÎncă nu există evaluări
- Asthma Guidelines: An Assessment of Physician Understanding and PracticeDocument7 paginiAsthma Guidelines: An Assessment of Physician Understanding and PracticeFilip ThorntonÎncă nu există evaluări
- Antipsychotic Treatment A Systematic Literature Review and Meta Analysis of Qualitative StudiesDocument12 paginiAntipsychotic Treatment A Systematic Literature Review and Meta Analysis of Qualitative StudiesmafeÎncă nu există evaluări
- Ms. Chithra Chandran A. First Year MSC Nursing Govt. College of Nursing KottayamDocument54 paginiMs. Chithra Chandran A. First Year MSC Nursing Govt. College of Nursing Kottayamchithrajayakrishnan100% (1)
- 2020 03 18 20038430v1 Full PDFDocument26 pagini2020 03 18 20038430v1 Full PDFpopov357Încă nu există evaluări
- Pharmacological Augmentation in Unipolar DepressionDocument39 paginiPharmacological Augmentation in Unipolar DepressionSusana Pérez ReyesÎncă nu există evaluări
- Murphy 2021Document11 paginiMurphy 2021okÎncă nu există evaluări
- Knowledge Attitudes and Barriers Towards Evidence Ba - 2017 - Hong Kong PhysioDocument9 paginiKnowledge Attitudes and Barriers Towards Evidence Ba - 2017 - Hong Kong PhysioAnuj ShandilyaÎncă nu există evaluări
- Dexamethasone For The Prevention of Postoperative Sore ThroatDocument9 paginiDexamethasone For The Prevention of Postoperative Sore Throatrfr vfrvfrfÎncă nu există evaluări
- Appendix G The Practice-Research Integration Project (Prip) A Student Manual A. DescriptionDocument9 paginiAppendix G The Practice-Research Integration Project (Prip) A Student Manual A. DescriptionMohan KumarÎncă nu există evaluări
- How Physicians Manage Medical Uncertainty: A Qualitative Study and Conceptual TaxonomyDocument17 paginiHow Physicians Manage Medical Uncertainty: A Qualitative Study and Conceptual TaxonomyAlexÎncă nu există evaluări
- Stepped Care Treatment Delivery For Depression: A Systematic Review and Meta-AnalysisDocument17 paginiStepped Care Treatment Delivery For Depression: A Systematic Review and Meta-AnalysisEtika Tunjung KencanaÎncă nu există evaluări
- Lam Et Al. (2020)Document13 paginiLam Et Al. (2020)VINICIUS CAMARGO KISSÎncă nu există evaluări
- A Pilot Study of Functional Cognitive Behavioral Therapy (FCBT) For SchizophreniaDocument9 paginiA Pilot Study of Functional Cognitive Behavioral Therapy (FCBT) For Schizophreniacamuss23Încă nu există evaluări
- Facilitated Pa-Depression-2Document13 paginiFacilitated Pa-Depression-2api-332791374Încă nu există evaluări
- Managing Low Pain: Attitudes and Treatment Preferences Physical TherapistsDocument8 paginiManaging Low Pain: Attitudes and Treatment Preferences Physical TherapistsSachin0808Încă nu există evaluări
- Knowledge Attitude and Practice Outcomes PDFDocument8 paginiKnowledge Attitude and Practice Outcomes PDFGhada ElhassanÎncă nu există evaluări
- Jurnal JiwaDocument6 paginiJurnal JiwaoldDEUSÎncă nu există evaluări
- What Phytotherapy Needs: Evidence Based Guidelines For Better Clinical PracticeDocument13 paginiWhat Phytotherapy Needs: Evidence Based Guidelines For Better Clinical PracticeLGMOQÎncă nu există evaluări
- 10 1111@jhn 12756Document10 pagini10 1111@jhn 12756Federico CilloÎncă nu există evaluări
- Oropharyngeal and Tongue Exercises (Myofunctional Therapy) For Snoring: A Systematic Review and Meta-AnalysisDocument7 paginiOropharyngeal and Tongue Exercises (Myofunctional Therapy) For Snoring: A Systematic Review and Meta-AnalysissirahÎncă nu există evaluări
- Complementary Therapies in Clinical PracticeDocument7 paginiComplementary Therapies in Clinical PracticeBkash ShahÎncă nu există evaluări
- Behavioral Therapies For Drug AbuseDocument15 paginiBehavioral Therapies For Drug AbuseAnkur BhatiaÎncă nu există evaluări
- Systematic Literature Review and Meta-Analysis of Medication Adherence With Once-Weekly Versus Once-Daily TherapyDocument10 paginiSystematic Literature Review and Meta-Analysis of Medication Adherence With Once-Weekly Versus Once-Daily Therapyb.modÎncă nu există evaluări
- CvaDocument10 paginiCvaapi-201999002Încă nu există evaluări
- IMRAD Format2Document33 paginiIMRAD Format2Juvy IringanÎncă nu există evaluări
- Carlozzi-14 RS Outcomes HDDocument20 paginiCarlozzi-14 RS Outcomes HDMARIA MONTSERRAT SOMOZA MONCADAÎncă nu există evaluări
- Predictors of Psych Intervention To Promote Health Behaviour Adherence in HF 2021Document14 paginiPredictors of Psych Intervention To Promote Health Behaviour Adherence in HF 2021Bob JoeÎncă nu există evaluări
- Allocation of Physician Time in Ambulatory Practice: A Time and Motion Study in 4 SpecialtiesDocument10 paginiAllocation of Physician Time in Ambulatory Practice: A Time and Motion Study in 4 SpecialtiesMonica CabaÎncă nu există evaluări
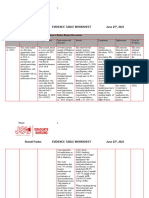
- BP DNP Evidence Table WorksheetDocument43 paginiBP DNP Evidence Table Worksheetapi-706947027Încă nu există evaluări
- Oup Accepted Manuscript 2020Document8 paginiOup Accepted Manuscript 2020Yusril AhmadÎncă nu există evaluări
- Bibliography: Science, 84-87Document3 paginiBibliography: Science, 84-87steffiÎncă nu există evaluări
- Magnitude of The Placebo Response Across Treatment Modalities Used For Treatment-Resistant Depression in Adults A Systematic Review and Meta-AnalysisDocument18 paginiMagnitude of The Placebo Response Across Treatment Modalities Used For Treatment-Resistant Depression in Adults A Systematic Review and Meta-AnalysisUSFMFPÎncă nu există evaluări
- 10 1016@j Neubiorev 2017 03 010Document24 pagini10 1016@j Neubiorev 2017 03 010USFMFPÎncă nu există evaluări
- 10 1016@j Arthro 2019 09 048Document6 pagini10 1016@j Arthro 2019 09 048USFMFPÎncă nu există evaluări
- Correlates of Generalized Anxiety Disorder: Independent of Co-Morbidity With DepressionDocument7 paginiCorrelates of Generalized Anxiety Disorder: Independent of Co-Morbidity With DepressionUSFMFPÎncă nu există evaluări
- 10.1016@s0016 50851732224 2Document1 pagină10.1016@s0016 50851732224 2USFMFPÎncă nu există evaluări
- Car 2509Document6 paginiCar 2509USFMFPÎncă nu există evaluări
- Accepted Manuscript: 10.1016/j.sleep.2018.03.031Document20 paginiAccepted Manuscript: 10.1016/j.sleep.2018.03.031USFMFPÎncă nu există evaluări
- 585Document15 pagini585USFMFPÎncă nu există evaluări
- Zhang 2015Document8 paginiZhang 2015USFMFPÎncă nu există evaluări
- Schizophr Bull 2015 Malhotra 1224 6Document3 paginiSchizophr Bull 2015 Malhotra 1224 6USFMFPÎncă nu există evaluări
- American Journal of Psychotherapy 2008 62, 1 Proquest CentralDocument33 paginiAmerican Journal of Psychotherapy 2008 62, 1 Proquest CentralUSFMFPÎncă nu există evaluări
- 10 1016@j Jemermed 2016 11 022Document7 pagini10 1016@j Jemermed 2016 11 022USFMFPÎncă nu există evaluări
- 10 1016@j Neuropsychologia 2016 09 020Document29 pagini10 1016@j Neuropsychologia 2016 09 020USFMFPÎncă nu există evaluări
- Edwards 2015Document9 paginiEdwards 2015USFMFPÎncă nu există evaluări
- 1 s2.0 S0149763415303481 MainDocument26 pagini1 s2.0 S0149763415303481 MainUSFMFPÎncă nu există evaluări
- Journal of Affective DisordersDocument11 paginiJournal of Affective DisordersUSFMFPÎncă nu există evaluări
- 1 s2.0 S0149763416301452 MainDocument50 pagini1 s2.0 S0149763416301452 MainUSFMFPÎncă nu există evaluări
- 10 1016@j Psychres 2016 09 028Document15 pagini10 1016@j Psychres 2016 09 028USFMFPÎncă nu există evaluări
- 1 s2.0 S0167945716300781 MainDocument11 pagini1 s2.0 S0167945716300781 MainUSFMFPÎncă nu există evaluări
- Background: Clinicaltrials - GovDocument10 paginiBackground: Clinicaltrials - GovUSFMFPÎncă nu există evaluări
- The Neurobehavioral and Molecular Phenotype of Angelman SyndromeDocument6 paginiThe Neurobehavioral and Molecular Phenotype of Angelman SyndromeUSFMFPÎncă nu există evaluări
- 1 s2.0 S1389945716300302 MainDocument27 pagini1 s2.0 S1389945716300302 MainUSFMFPÎncă nu există evaluări
- 1 s2.0 S0165032715311721 MainDocument6 pagini1 s2.0 S0165032715311721 MainUSFMFPÎncă nu există evaluări
- Comprehensive PsychiatryDocument24 paginiComprehensive PsychiatryUSFMFPÎncă nu există evaluări
- 10.0000@graphics - Tx.ovid - Com@generic 7AEFD8507F7EDocument8 pagini10.0000@graphics - Tx.ovid - Com@generic 7AEFD8507F7EUSFMFPÎncă nu există evaluări
- 1 s2.0 S0010440X15303175 MainDocument20 pagini1 s2.0 S0010440X15303175 MainUSFMFPÎncă nu există evaluări
- Comprehensive PsychiatryDocument27 paginiComprehensive PsychiatryUSFMFPÎncă nu există evaluări
- BR J Soc Work 2007 Preece 925 36Document12 paginiBR J Soc Work 2007 Preece 925 36USFMFPÎncă nu există evaluări
- Practice: Social Work in ActionDocument17 paginiPractice: Social Work in ActionUSFMFPÎncă nu există evaluări
- Midwifery Drug Administration ExamDocument7 paginiMidwifery Drug Administration ExamteabagmanÎncă nu există evaluări
- Pharmacokinetics Pharmacodynamics of Controlled Release SystemsDocument33 paginiPharmacokinetics Pharmacodynamics of Controlled Release SystemsSumant SainiÎncă nu există evaluări
- Marketing Plan B6 BioconDocument9 paginiMarketing Plan B6 BioconRitvik DineshÎncă nu există evaluări
- 1.history of Drugs and Dosage FormsDocument23 pagini1.history of Drugs and Dosage FormsMùkhtæær Ïbňü ÅhmēdÎncă nu există evaluări
- antimicrobial agents تجميعيDocument5 paginiantimicrobial agents تجميعيahmedmahmoudfelefil93Încă nu există evaluări
- MannitolDocument2 paginiMannitolRyan OnellÎncă nu există evaluări
- Flag Medicines - Inventory 04-Apr-2023Document30 paginiFlag Medicines - Inventory 04-Apr-2023Luis Alfredo Dominguez MoralesÎncă nu există evaluări
- London Cancer Mesna Guideline v1Document8 paginiLondon Cancer Mesna Guideline v1Nurkholis AminÎncă nu există evaluări
- Ashwini 1Document13 paginiAshwini 1Swagath NÎncă nu există evaluări
- AmitriptylineDocument9 paginiAmitriptylinetrimi68Încă nu există evaluări
- Corp - 253.1 - Paediatric FormularyDocument530 paginiCorp - 253.1 - Paediatric FormularySamith AlvaÎncă nu există evaluări
- Growing Portfolio of Complex InjectablesDocument4 paginiGrowing Portfolio of Complex InjectablesTathagata DuttaÎncă nu există evaluări
- Monteleone - Marx 2000 PRP Vs Thrombin in Skin Graft Donor Site RepairDocument2 paginiMonteleone - Marx 2000 PRP Vs Thrombin in Skin Graft Donor Site RepairViviane KaramÎncă nu există evaluări
- Quality Information SummaryDocument3 paginiQuality Information SummaryHenry Kay100% (1)
- Hypersalivation - What Drug Treatment Options Are Available?Document5 paginiHypersalivation - What Drug Treatment Options Are Available?Kanwal NafisÎncă nu există evaluări
- Lactulose Drug StudyDocument1 paginăLactulose Drug StudyJhanine ArellanoÎncă nu există evaluări
- Formoterol Gonzaga.Document2 paginiFormoterol Gonzaga.Sheryl Anne GonzagaÎncă nu există evaluări
- Your Role in Code BlueDocument26 paginiYour Role in Code BlueZeny Orpilla Gok-ongÎncă nu există evaluări
- Soal Teks ReportDocument3 paginiSoal Teks ReportArmia FebrianaÎncă nu există evaluări
- Form DDDDocument11 paginiForm DDDAdhelia Aksti PertiwiÎncă nu există evaluări
- Preparation and Evaluation of Immediate Release TabletsDocument9 paginiPreparation and Evaluation of Immediate Release TabletsEditor IJTSRDÎncă nu există evaluări
- SedativeDocument15 paginiSedativeManul ShobujÎncă nu există evaluări
- Mod3 (Manor) Disp-AdrDocument18 paginiMod3 (Manor) Disp-AdrGizelle CorpuzÎncă nu există evaluări
- 7.2023 HSIC Vietnam DCB Complex LHB Draft3 FDocument32 pagini7.2023 HSIC Vietnam DCB Complex LHB Draft3 FR&D DepartmentÎncă nu există evaluări
- Antidepressant and Antipsychotic Side-Effects and Personalised Prescribing, A Systematic Review and Digital Tool Development. Lancet 2023Document17 paginiAntidepressant and Antipsychotic Side-Effects and Personalised Prescribing, A Systematic Review and Digital Tool Development. Lancet 2023tomil.hoÎncă nu există evaluări
- Daftar Obat Lasa: Nama Obat Sama Kekuatan BedaDocument2 paginiDaftar Obat Lasa: Nama Obat Sama Kekuatan BedaTut RaiÎncă nu există evaluări
- Korelasi Posisi Tip Catheter Double Lumen Dengan Nilai Quick of Blood Pada Pemasangan CDL Tunneling Vena Jugularis Interna Kanan Di RSUP Prof. Dr. R. D. KandouDocument6 paginiKorelasi Posisi Tip Catheter Double Lumen Dengan Nilai Quick of Blood Pada Pemasangan CDL Tunneling Vena Jugularis Interna Kanan Di RSUP Prof. Dr. R. D. KandoutandiÎncă nu există evaluări
- Community Pharmacy III Training Manual (0201463)Document37 paginiCommunity Pharmacy III Training Manual (0201463)Khairi Mustafa SalemÎncă nu există evaluări
- The New Advanced Cardiac Life Support GuidelinesDocument52 paginiThe New Advanced Cardiac Life Support GuidelinesFandy Hazzy AlfataÎncă nu există evaluări
- Master List of Prescription Abbreviations: Abbreviation From The Latin MeaningDocument4 paginiMaster List of Prescription Abbreviations: Abbreviation From The Latin Meaning_Junz_0% (1)