S-ar putea să vă placă și
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesDe la EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesEvaluare: 4 din 5 stele4/5 (6)
- ACLS Algorithms 2020 (Advanced Cardiac Life Support)Document1 paginăACLS Algorithms 2020 (Advanced Cardiac Life Support)evelyn k100% (2)
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesDe la EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesEvaluare: 5 din 5 stele5/5 (2)
- Icu Cheat Sheet Working FileDocument7 paginiIcu Cheat Sheet Working FileBhumiShahÎncă nu există evaluări
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideDe la EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideÎncă nu există evaluări
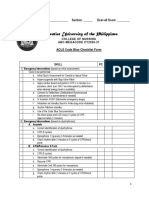
- ABC ACLS Checklist Online CY2020 21Document8 paginiABC ACLS Checklist Online CY2020 21Anastasya Gishella RorongÎncă nu există evaluări
- PALS Algorithms 2019 (Pediatric Advanced Life Support)Document1 paginăPALS Algorithms 2019 (Pediatric Advanced Life Support)darlingcarvajalduqueÎncă nu există evaluări
- Pediatric Anesthesiology - A Comprehensive Board Review, 1st Ed - 2015Document713 paginiPediatric Anesthesiology - A Comprehensive Board Review, 1st Ed - 2015linwet100% (6)
- A Guide To ConsultsDocument36 paginiA Guide To ConsultsspamvarunÎncă nu există evaluări
- Emergency Department Intubation ChecklisTDocument2 paginiEmergency Department Intubation ChecklisTStacey Woods100% (1)
- Using The ACLS Primary Survey For A Patient in Respiratory ArrestDocument34 paginiUsing The ACLS Primary Survey For A Patient in Respiratory Arrest강기연100% (1)
- Anaesthesia in Obese PatientsDocument72 paginiAnaesthesia in Obese PatientsPraveen RamasamyÎncă nu există evaluări
- PQ1Document50 paginiPQ1명수김100% (1)
- Peri Operative NursingDocument184 paginiPeri Operative Nursingfelxhu100% (3)
- 2011 Monitoring in Anesthesia and Perioperative CareDocument437 pagini2011 Monitoring in Anesthesia and Perioperative CareOskar MartinezÎncă nu există evaluări
- Nurses NotesDocument1 paginăNurses Notesmona_javier100% (4)
- Nicu Survival Guide For ResidentsDocument26 paginiNicu Survival Guide For ResidentspeppepagÎncă nu există evaluări
- Stanford Clinical Anesthesia TextbookDocument103 paginiStanford Clinical Anesthesia TextbookRishi Sharma100% (2)
- Perioperative Reda Harby NotesDocument23 paginiPerioperative Reda Harby NotesSazzad100% (2)
- Rapid Sequence Intubation ReportDocument55 paginiRapid Sequence Intubation Reportlorkan19100% (1)
- P1 LONG EXAM Block 1 NUR104 Nursing Health Ethics BioethicsDocument44 paginiP1 LONG EXAM Block 1 NUR104 Nursing Health Ethics Bioethicsella retizaÎncă nu există evaluări
- Acapella ProtocolDocument3 paginiAcapella ProtocolRTdadÎncă nu există evaluări
- Mechanical Ventilation in NeonatesDocument60 paginiMechanical Ventilation in NeonatesZuhair Aldajani زهير عمر الدجاني100% (3)
- Sizing Medical Gas Piping - Archives - PMEngineerDocument3 paginiSizing Medical Gas Piping - Archives - PMEngineerSaif MohammadÎncă nu există evaluări
- ETT IntubationDocument27 paginiETT IntubationGilbert Sterling Octavius100% (1)
- Bipap Ventilation Basic and MonitoringDocument33 paginiBipap Ventilation Basic and MonitoringPradip ChougaleÎncă nu există evaluări
- Intubation ChecklistDocument2 paginiIntubation ChecklistDaniel CrookÎncă nu există evaluări
- Medical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 22Document16 paginiMedical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 22sarasjunkÎncă nu există evaluări
- Staffing in Ot and Members of Surgical TeamDocument4 paginiStaffing in Ot and Members of Surgical Teamvinnu kalyan50% (2)
- Drug-Assisted Intubation (Dai) : Expanded Scope Practice (NR)Document1 paginăDrug-Assisted Intubation (Dai) : Expanded Scope Practice (NR)MEKSELINA KALENDERÎncă nu există evaluări
- Rapid Sequence Intubation W Checklist 2022Document4 paginiRapid Sequence Intubation W Checklist 2022drulilalbbÎncă nu există evaluări
- Econdary ABCD (Airway, Breathing, Circulation, Differential Diagnosis)Document20 paginiEcondary ABCD (Airway, Breathing, Circulation, Differential Diagnosis)Nikol NataliaÎncă nu există evaluări
- PALS Guidelines For HypotensionDocument19 paginiPALS Guidelines For HypotensionAnil SharmaÎncă nu există evaluări
- Rapid Sequence Intubation PMGDocument3 paginiRapid Sequence Intubation PMGjaggaÎncă nu există evaluări
- N.C.M. 106 Preliminary Exams Reviewer: Nyjil Patrick B. ColumbresDocument11 paginiN.C.M. 106 Preliminary Exams Reviewer: Nyjil Patrick B. ColumbresNyjil Patrick Basilio ColumbresÎncă nu există evaluări
- Weingart Vent HandoutDocument4 paginiWeingart Vent HandoutStrept Pneumonia100% (1)
- General Anesthesia: IntubationDocument44 paginiGeneral Anesthesia: IntubationMiezu CosminÎncă nu există evaluări
- Induced SputumDocument6 paginiInduced Sputumnh2411Încă nu există evaluări
- BiPAP ManyDocument47 paginiBiPAP ManyHarshit RastogiÎncă nu există evaluări
- Airway / Breathing ProtocolsDocument15 paginiAirway / Breathing ProtocolsSbarcea AurelÎncă nu există evaluări
- Vent ProtocolDocument15 paginiVent Protocolihtisham1Încă nu există evaluări
- Airway Management - AlgorithmeDocument1 paginăAirway Management - AlgorithmeagungpratamaputraÎncă nu există evaluări
- Nursing Care PlanDocument8 paginiNursing Care PlanAngela SweetÎncă nu există evaluări
- Ccu NotesDocument76 paginiCcu NotesAr PeeÎncă nu există evaluări
- Special ProceduresDocument9 paginiSpecial ProceduresKate AbellaÎncă nu există evaluări
- Surfactant Final 2Document5 paginiSurfactant Final 2anuÎncă nu există evaluări
- Assignment ON Advanced Cardiac Life Support: Submitted To: Submitted byDocument7 paginiAssignment ON Advanced Cardiac Life Support: Submitted To: Submitted byAnanthibalaÎncă nu există evaluări
- OVERVIEW Rapid Sequence Intubation (RSI) Is An Airway Management Technique That ProducesDocument7 paginiOVERVIEW Rapid Sequence Intubation (RSI) Is An Airway Management Technique That ProducesOkami PÎncă nu există evaluări
- Basic Life SupportDocument34 paginiBasic Life SupportEveline FebrinaÎncă nu există evaluări
- Laparoscopic Sleeve Gastrictomy DictationDocument3 paginiLaparoscopic Sleeve Gastrictomy DictationHassanÎncă nu există evaluări
- 4.assignment On Endo TubeDocument5 pagini4.assignment On Endo Tubesantosh kumarÎncă nu există evaluări
- ALS-Adult All ProtocolsDocument54 paginiALS-Adult All ProtocolsNur SusiawantyÎncă nu există evaluări
- Adult NasalDocument14 paginiAdult NasalillirpohnimÎncă nu există evaluări
- Respiratory Distress/Failure Scenario: General Code OutlineDocument2 paginiRespiratory Distress/Failure Scenario: General Code OutlineLpa LV Tumbleweeds ChapterÎncă nu există evaluări
- BipapDocument26 paginiBipapالغائب الحاضرÎncă nu există evaluări
- Induced HPDocument4 paginiInduced HPmaddythedocÎncă nu există evaluări
- Tabije, Arvie Jayselle PDocument8 paginiTabije, Arvie Jayselle PJaysellePuguonTabijeÎncă nu există evaluări
- Pediatric Anesthesia Manual: A.Matveevskii, S.White Second EditionDocument49 paginiPediatric Anesthesia Manual: A.Matveevskii, S.White Second EditionMauricio PinneaparÎncă nu există evaluări
- No. 10 SANAANI Topic For Esophagogastric Balloon Tamponade Tubes Billroth 1 and 11Document12 paginiNo. 10 SANAANI Topic For Esophagogastric Balloon Tamponade Tubes Billroth 1 and 11Nur SanaaniÎncă nu există evaluări
- DR - Rajalakshmi.C: Emergency Physician MMHRC Institute of Emergency MedicineDocument22 paginiDR - Rajalakshmi.C: Emergency Physician MMHRC Institute of Emergency MedicineP Vinod KumarÎncă nu există evaluări
- Indications For Intubation and RSIDocument52 paginiIndications For Intubation and RSIchenn1992Încă nu există evaluări
- ITU Handbook For Non-Anaesthetists 214Document23 paginiITU Handbook For Non-Anaesthetists 214AtikaÎncă nu există evaluări
- Surgery and Perioperative Care: AnaestheticsDocument146 paginiSurgery and Perioperative Care: Anaestheticsjames.a.blairÎncă nu există evaluări
- OBcheetsheetDocument6 paginiOBcheetsheetapi-3807143Încă nu există evaluări
- AlgorithmACLS CA COVID LNGDSCRP 220203Document3 paginiAlgorithmACLS CA COVID LNGDSCRP 220203AndhikaÎncă nu există evaluări
- Jawt 11 I 1 P 1Document6 paginiJawt 11 I 1 P 1Jesicca SÎncă nu există evaluări
- Endotracheal IntubationDocument28 paginiEndotracheal Intubationjeevan ghimireÎncă nu există evaluări
- Vent v1 Tom Extubation 001-EnDocument4 paginiVent v1 Tom Extubation 001-EnMuhammad AleemÎncă nu există evaluări
- Airway Management in TransportDocument46 paginiAirway Management in TransportArtha PutuÎncă nu există evaluări
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYDe la EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYÎncă nu există evaluări
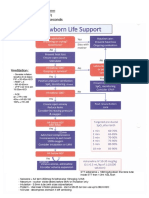
- Vigorous Drying!!!!!! - Ax: Tone, HR, RR - Re-Ax Every 30secondsDocument1 paginăVigorous Drying!!!!!! - Ax: Tone, HR, RR - Re-Ax Every 30secondsspamvarunÎncă nu există evaluări
- PDF Anaesthetic Drugs1 PDFDocument2 paginiPDF Anaesthetic Drugs1 PDFspamvarunÎncă nu există evaluări
- EU Anaesthesia Training Program Curriculum V1 6c 20170612 Appendix 3Document13 paginiEU Anaesthesia Training Program Curriculum V1 6c 20170612 Appendix 3spamvarunÎncă nu există evaluări
- 2018 ICU SRMO Critical CareDocument10 pagini2018 ICU SRMO Critical CarespamvarunÎncă nu există evaluări
- Combined Flyer&Registration 2015Document3 paginiCombined Flyer&Registration 2015spamvarunÎncă nu există evaluări
- Training Accreditation Handbook PDFDocument234 paginiTraining Accreditation Handbook PDFspamvarunÎncă nu există evaluări
- 2010 FeesDocument2 pagini2010 FeesspamvarunÎncă nu există evaluări
- Modifier CEU TestDocument11 paginiModifier CEU TestLaureen JandroepÎncă nu există evaluări
- The Central and Peripheral Effects of The Methanol Extract of Fadogia Cienkowskii Schweinf. Var Cienkowskii LeavesDocument6 paginiThe Central and Peripheral Effects of The Methanol Extract of Fadogia Cienkowskii Schweinf. Var Cienkowskii LeavesIOSRjournalÎncă nu există evaluări
- Anaesthesia in Dogs and Cats With Cardiac DiseaseDocument19 paginiAnaesthesia in Dogs and Cats With Cardiac DiseaseALEJANDRA MADRIGALÎncă nu există evaluări
- Drug Name Mechanism of Action Indication Contraindication Side Effects/ Adverse Effects Nursing Considerations Generic Name Oxytocin Side EffectsDocument15 paginiDrug Name Mechanism of Action Indication Contraindication Side Effects/ Adverse Effects Nursing Considerations Generic Name Oxytocin Side EffectsRomwella May AlgoÎncă nu există evaluări
- Soluzioni IngleseDocument239 paginiSoluzioni IngleseAxel BlazeÎncă nu există evaluări
- Module 1 Case StudyDocument7 paginiModule 1 Case StudyDivine ParagasÎncă nu există evaluări
- Preoperative AssessmentDocument3 paginiPreoperative AssessmentStepyn SalvadorÎncă nu există evaluări
- Rguhs Oral SurgeryDocument9 paginiRguhs Oral SurgerydrpnnreddyÎncă nu există evaluări
- Anaesthetic Challenges and Management of Myelomeningocele RepairDocument6 paginiAnaesthetic Challenges and Management of Myelomeningocele RepairprastiaÎncă nu există evaluări
- Analgesic Efficacy of Erector Spinae Plane BlocksDocument7 paginiAnalgesic Efficacy of Erector Spinae Plane BlocksAlejandra SanchezÎncă nu există evaluări
- 1.introduction To Anesthesiology CSU CMS LectureDocument26 pagini1.introduction To Anesthesiology CSU CMS LectureKenneth MiguelÎncă nu există evaluări
- Group 5 Pubmed Accepted Results PDFDocument683 paginiGroup 5 Pubmed Accepted Results PDFDnyanesh LimayeÎncă nu există evaluări
- Nursing Management of During Stages of Labor and Delivery UpdatedDocument60 paginiNursing Management of During Stages of Labor and Delivery UpdatedSherlyn Miranda GarcesÎncă nu există evaluări
- 207Document5 pagini207Satria 'arceus' DewantaraÎncă nu există evaluări
- مقاصة ٢Document9 paginiمقاصة ٢tahahagag99Încă nu există evaluări
- Simulation-Consent For SurgicalDocument2 paginiSimulation-Consent For SurgicalMargaret Barco DeanesÎncă nu există evaluări
- Chapter 16 - Comfort Measures During Labor and Birth: Ob LectureDocument6 paginiChapter 16 - Comfort Measures During Labor and Birth: Ob LectureLyndon SayongÎncă nu există evaluări
- Question Bank (Pharmacology) Paper No-1 (CNS) : Name The FollowingDocument25 paginiQuestion Bank (Pharmacology) Paper No-1 (CNS) : Name The FollowingAdarshBijapurÎncă nu există evaluări
- Uganda Charitable Spine Surgery Mission 2013 Trip Report Ver 1 Sept 15Document29 paginiUganda Charitable Spine Surgery Mission 2013 Trip Report Ver 1 Sept 15api-197209808Încă nu există evaluări
- ACTES Programme PDFDocument29 paginiACTES Programme PDFandreaÎncă nu există evaluări