S-ar putea să vă placă și
- FRCPath OSPE 25042014Document11 paginiFRCPath OSPE 25042014monday125Încă nu există evaluări
- Part 1 SAQs Specimen QuestionsDocument79 paginiPart 1 SAQs Specimen Questionsخولة رشيد العيسى100% (2)
- FRCPath Mock 2014 Model AnswersDocument29 paginiFRCPath Mock 2014 Model Answersmonday125Încă nu există evaluări
- OspeDocument29 paginiOspemonday125Încă nu există evaluări
- Medicine IMM SyllabusDocument53 paginiMedicine IMM SyllabusAamir HamaadÎncă nu există evaluări
- Code of Ethics Guidance DocumentDocument30 paginiCode of Ethics Guidance DocumentASHVINBHAI VACHHANI100% (1)
- Chemical Pathology HODocument17 paginiChemical Pathology HOMurali TiarasanÎncă nu există evaluări
- Chemical Pathology Workshop II - Diagnostic Theory in Chemical Pathology (2017.11.14)Document57 paginiChemical Pathology Workshop II - Diagnostic Theory in Chemical Pathology (2017.11.14)Arthur Chang100% (1)
- Chemical Pathology II HIV AIDSDocument33 paginiChemical Pathology II HIV AIDSSimeon AdebisiÎncă nu există evaluări
- Routine and Acute Clinical ChemistryDocument2 paginiRoutine and Acute Clinical ChemistryMohamed MounirÎncă nu există evaluări
- Microsoft Power Point - FRCPath Practical Exam 2009 WebsiteDocument20 paginiMicrosoft Power Point - FRCPath Practical Exam 2009 Websitesakai33100% (1)
- Simulation StationDocument2 paginiSimulation Stationmonday125Încă nu există evaluări
- Methods Comparison 5th Sept'18 DR PriyaDocument65 paginiMethods Comparison 5th Sept'18 DR Priyaamit danielÎncă nu există evaluări
- Laboratory Tests For EndocrinologyDocument6 paginiLaboratory Tests For EndocrinologyAnastasia100% (1)
- Chemical Pathology Stage A Examination Sample QuestionsDocument10 paginiChemical Pathology Stage A Examination Sample QuestionsHabib UllahÎncă nu există evaluări
- IFCC TF Ethics in Lab MedicineDocument16 paginiIFCC TF Ethics in Lab MedicineDr.Deepanshu SinghalÎncă nu există evaluări
- Karen Smith Duty Biochemist ScenariosDocument43 paginiKaren Smith Duty Biochemist Scenariosmonday125100% (2)
- DR Cole Storage Disorders Hand OutDocument3 paginiDR Cole Storage Disorders Hand Outmonday125Încă nu există evaluări
- DR Moat Paediatric BochemistryDocument62 paginiDR Moat Paediatric Bochemistrymonday125Încă nu există evaluări
- Chemical Pathology Job Description December 2011Document9 paginiChemical Pathology Job Description December 2011Chengyuan ZhangÎncă nu există evaluări
- Wet Practical Frcpath2014Document7 paginiWet Practical Frcpath2014monday125Încă nu există evaluări
- Scientist Viva AnswerDocument2 paginiScientist Viva Answermonday125Încă nu există evaluări
- Acid-Base MSC CasesDocument16 paginiAcid-Base MSC Casesmonday125Încă nu există evaluări
- Plasma Enzyme DiagnosisDocument30 paginiPlasma Enzyme DiagnosisKayode IbitoyeÎncă nu există evaluări
- Case Study Analysis (1,2,3,4) ENDOCRINOLOGYDocument3 paginiCase Study Analysis (1,2,3,4) ENDOCRINOLOGYDayledaniel Sorveto100% (1)
- FOCUS SAS Training Day Leeds Dr. Joanna Sheldon Protein Reference Unit, St. George'sDocument19 paginiFOCUS SAS Training Day Leeds Dr. Joanna Sheldon Protein Reference Unit, St. George'smonday125Încă nu există evaluări
- Tests Affected by Haemolysed, Icteric and Lipemic Samples, W5-SOP-1-1-1Document2 paginiTests Affected by Haemolysed, Icteric and Lipemic Samples, W5-SOP-1-1-1Dejan BodetićÎncă nu există evaluări
- Laboratorial Diagnostics Keypoints RevisionDocument6 paginiLaboratorial Diagnostics Keypoints RevisionFathimathÎncă nu există evaluări
- Critical Appraisal: DR A C J Hutchesson Chair of Examiners' Panel, Frcpath (Clinical Biochemistry)Document10 paginiCritical Appraisal: DR A C J Hutchesson Chair of Examiners' Panel, Frcpath (Clinical Biochemistry)monday125Încă nu există evaluări
- A Review of Medical Errors in Laboratory Diagnostics and Where We Are TodayDocument4 paginiA Review of Medical Errors in Laboratory Diagnostics and Where We Are TodaytaghamdÎncă nu există evaluări
- COMPILED SCTL Adrenal Disorders PDFDocument14 paginiCOMPILED SCTL Adrenal Disorders PDFeeelie35Încă nu există evaluări
- Introduction of Clinical BiochemistryDocument32 paginiIntroduction of Clinical BiochemistryKaren LowÎncă nu există evaluări
- Heat Coagulation TestDocument8 paginiHeat Coagulation TestRawan MaherÎncă nu există evaluări
- ICP-MS Talk ACBDocument31 paginiICP-MS Talk ACBmonday125Încă nu există evaluări
- Quality Control in Clinical Biochemistry BMLTDocument56 paginiQuality Control in Clinical Biochemistry BMLTSelim JaforÎncă nu există evaluări
- Quality Control2Document32 paginiQuality Control2Mustafa KhandgawiÎncă nu există evaluări
- Prenatal Diagnosis (Brynn Levy)Document357 paginiPrenatal Diagnosis (Brynn Levy)Pranali PatelÎncă nu există evaluări
- JIPMER Residents ManualDocument68 paginiJIPMER Residents ManualSaroj PandaÎncă nu există evaluări
- 2.5 Antibody ScreeningDocument5 pagini2.5 Antibody ScreeningBALAJIÎncă nu există evaluări
- Critical Value in HematologyDocument8 paginiCritical Value in HematologySTARK DIAGNOSTICSÎncă nu există evaluări
- Laboratory Turnaround TimeDocument17 paginiLaboratory Turnaround TimeNicole HoÎncă nu există evaluări
- Toxicology and TDMDocument121 paginiToxicology and TDMteppie0917Încă nu există evaluări
- Clinical ChemistryDocument333 paginiClinical ChemistryshooberÎncă nu există evaluări
- CBC Lecture For NehouaDocument68 paginiCBC Lecture For NehouaErmal Beqiraj100% (1)
- Liver Function Test: Prepared By: Siti Norhaiza Binti HadzirDocument33 paginiLiver Function Test: Prepared By: Siti Norhaiza Binti Hadzirmhafiziab100% (1)
- BMED425 20130926124157 SyllabusDocument8 paginiBMED425 20130926124157 Syllabusahmad0% (1)
- BiochemistryDocument135 paginiBiochemistryPradip HamalÎncă nu există evaluări
- Alpha Fetoprotein (Afp)Document10 paginiAlpha Fetoprotein (Afp)Andi UkengÎncă nu există evaluări
- Shelly HyperlipidemiaDocument22 paginiShelly Hyperlipidemiaale marilÎncă nu există evaluări
- MCQs TOXICOLOGYEXAMPLESDocument15 paginiMCQs TOXICOLOGYEXAMPLESesraaÎncă nu există evaluări
- Clinical Biochemistry Reference Ranges HandbookDocument18 paginiClinical Biochemistry Reference Ranges HandbookMurali DathanÎncă nu există evaluări
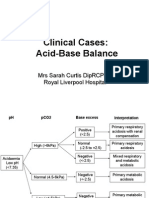
- Assessment Disorders Acidbase Sarah CurtisDocument39 paginiAssessment Disorders Acidbase Sarah Curtismonday125100% (1)
- Routine Laboratory Evaluation of CoagulationDocument7 paginiRoutine Laboratory Evaluation of CoagulationGilo IlaganÎncă nu există evaluări
- Biochemical Tests in Diabetes: DR Joe Fleming PHD MCB Frcpath Dept of Clinical Biochemistry CMC VelloreDocument43 paginiBiochemical Tests in Diabetes: DR Joe Fleming PHD MCB Frcpath Dept of Clinical Biochemistry CMC Velloremariya khanÎncă nu există evaluări
- Lipid Profile: by Micheal and ChristianDocument15 paginiLipid Profile: by Micheal and ChristianMichealÎncă nu există evaluări
- Ovarian Reserve Testing and Follicular MonitoringDocument35 paginiOvarian Reserve Testing and Follicular Monitoringjindal clinicsÎncă nu există evaluări
- Clinical Lab TechnqDocument67 paginiClinical Lab TechnqRatnamala SarmaÎncă nu există evaluări
- Manchester Anaemia GuideDocument13 paginiManchester Anaemia Guidemubzy14Încă nu există evaluări
- Ab CD EfDocument28 paginiAb CD EfDurgaNadella100% (1)
- EczemaDocument21 paginiEczemaLil_QuinceÎncă nu există evaluări
- Randomized Controlled Multicentre Study of Albumin Replacement Therapy in Septic Shock (ARISS) : Protocol For A Randomized Controlled TrialDocument13 paginiRandomized Controlled Multicentre Study of Albumin Replacement Therapy in Septic Shock (ARISS) : Protocol For A Randomized Controlled TrialntnquynhproÎncă nu există evaluări
- The 2030 Agenda For Sustainable Development and The "Five PS"Document2 paginiThe 2030 Agenda For Sustainable Development and The "Five PS"Laraib ShahidÎncă nu există evaluări
- Parkinsonism A General Motor Disability PDFDocument9 paginiParkinsonism A General Motor Disability PDFRishabh SinghÎncă nu există evaluări
- NVS q1 2017 Ir PresentationDocument122 paginiNVS q1 2017 Ir PresentationmedtechyÎncă nu există evaluări
- Local Food Trade Shows ProgramDocument39 paginiLocal Food Trade Shows ProgramAmy KleinÎncă nu există evaluări
- Medical Device Adverse Event Reporting Form: Materiovigilance Programme of India (Mvpi)Document4 paginiMedical Device Adverse Event Reporting Form: Materiovigilance Programme of India (Mvpi)ashwani niteshÎncă nu există evaluări
- Co-Occurring Disorders: Substance Use and Mental HealthDocument52 paginiCo-Occurring Disorders: Substance Use and Mental HealthElisyah MarsiahÎncă nu există evaluări
- Kirloskar Brothers Limited, KirloskarvadiDocument71 paginiKirloskar Brothers Limited, KirloskarvadiNilesh JadhavÎncă nu există evaluări
- Unit4 Planning For A Health CareerDocument76 paginiUnit4 Planning For A Health CareerkitcathÎncă nu există evaluări
- Own: ICARUS Training Services Safety Briefing/ Attendance FormDocument2 paginiOwn: ICARUS Training Services Safety Briefing/ Attendance FormTim Brown0% (1)
- Antimicrobial Screen - Dub DiolDocument4 paginiAntimicrobial Screen - Dub DiolNgân BảoÎncă nu există evaluări
- 11 Benefits of Competitive Sports For Kids and AdultsDocument8 pagini11 Benefits of Competitive Sports For Kids and AdultsNguyễn Kiều ThanhÎncă nu există evaluări
- KAR Products - Gloss White Aerosol PaintDocument7 paginiKAR Products - Gloss White Aerosol Paintjaredf@jfelectric.comÎncă nu există evaluări
- Population ExplosionDocument4 paginiPopulation ExplosionMonika KhariÎncă nu există evaluări
- Mapeh 10 Second Quarter ExamDocument3 paginiMapeh 10 Second Quarter ExamLILYBETH QUEMADA0% (1)
- 1 SM PDFDocument4 pagini1 SM PDFUtibe Tibz IkpembeÎncă nu există evaluări
- Contoh Daftar Belanja Obat Praktek PribadiDocument10 paginiContoh Daftar Belanja Obat Praktek PribadimeryÎncă nu există evaluări
- Complementary Feeding in Infants: An Ayurvedic Overview: ArticleDocument7 paginiComplementary Feeding in Infants: An Ayurvedic Overview: ArticleRadhika RÎncă nu există evaluări
- Inguinal Abscess Following CastrationDocument2 paginiInguinal Abscess Following Castrationfahmi rosyadiÎncă nu există evaluări
- Healthcare System of PakistanDocument7 paginiHealthcare System of PakistanHamza IshtiaqÎncă nu există evaluări
- Vasculitis SyndromesDocument56 paginiVasculitis SyndromesHengki Permana PutraÎncă nu există evaluări
- CNA Body Mechanics Bed Making Comfort CareDocument32 paginiCNA Body Mechanics Bed Making Comfort CareFaith VaughnÎncă nu există evaluări
- Black SigatokaDocument2 paginiBlack SigatokaLALUKISÎncă nu există evaluări
- Call Letter Specimen 2021 2022Document4 paginiCall Letter Specimen 2021 2022Dr SahibaÎncă nu există evaluări
- Asma Dan COPDDocument52 paginiAsma Dan COPDErik II100% (1)
- Strategic Plan 2023Document12 paginiStrategic Plan 2023BernewsAdminÎncă nu există evaluări
- Drug List 1Document2 paginiDrug List 1Ezra Lee NgatiyonÎncă nu există evaluări
- Atherosclerosis and Ischemic Heart Disease: UtlineDocument8 paginiAtherosclerosis and Ischemic Heart Disease: UtlinevmdcabanillaÎncă nu există evaluări
- MT-Mental Health-JMTDocument29 paginiMT-Mental Health-JMTLuis AlbertoÎncă nu există evaluări