S-ar putea să vă placă și
- Catastrophe Claims Guide 2007Document163 paginiCatastrophe Claims Guide 2007cottchen6605100% (1)
- A Child Presenting With Visual Impairment 28/4/2020Document40 paginiA Child Presenting With Visual Impairment 28/4/2020Sindhu BabuÎncă nu există evaluări
- Childhood BlindnessDocument14 paginiChildhood BlindnessAditya Arya PutraÎncă nu există evaluări
- Myopia by NamanDocument19 paginiMyopia by NamanAkshit ChitkaraÎncă nu există evaluări
- Research ProposalDocument45 paginiResearch ProposalAaliyah Marie AbaoÎncă nu există evaluări
- Guidelines For Prescribing EyeglassesDocument18 paginiGuidelines For Prescribing Eyeglassesratujelita100% (1)
- Eye Disorder in Childhood & Adolescent: Lia Meuthia Zaini FK Unsyiah / RSUZADocument54 paginiEye Disorder in Childhood & Adolescent: Lia Meuthia Zaini FK Unsyiah / RSUZACut MulianiÎncă nu există evaluări
- Nielsen & Co., Inc. v. Lepanto Consolidated Mining Co., 34 Phil, 122 (1915)Document3 paginiNielsen & Co., Inc. v. Lepanto Consolidated Mining Co., 34 Phil, 122 (1915)Abby PajaronÎncă nu există evaluări
- Macular Degeneration: A Complete Guide for Patients and Their FamiliesDe la EverandMacular Degeneration: A Complete Guide for Patients and Their FamiliesEvaluare: 5 din 5 stele5/5 (1)
- Atul Bisht Research Project ReportDocument71 paginiAtul Bisht Research Project ReportAtul BishtÎncă nu există evaluări
- Accounting 110: Acc110Document19 paginiAccounting 110: Acc110ahoffm05100% (1)
- Childhood GlaucomaDocument60 paginiChildhood Glaucomaeyemd_in_training100% (1)
- Retinopathy of PrematurityDocument16 paginiRetinopathy of PrematurityCzarina Mae LomboyÎncă nu există evaluări
- Can A Preterm Birth Cause Myopia? How?Document7 paginiCan A Preterm Birth Cause Myopia? How?mk26qb7gcbÎncă nu există evaluări
- MEHT130423 - Information For Screening For Retinopathy of Prematurity 1.0Document4 paginiMEHT130423 - Information For Screening For Retinopathy of Prematurity 1.0Rohit BharadwajÎncă nu există evaluări
- Retinopathy of PrematurityDocument15 paginiRetinopathy of Prematuritymarissa ulkhairÎncă nu există evaluări
- Retinopathy of Prematurity Like Retinopathy in Full-Term InfantsDocument9 paginiRetinopathy of Prematurity Like Retinopathy in Full-Term InfantsReza SatriaÎncă nu există evaluări
- Rop 2014Document13 paginiRop 2014mp1a1234Încă nu există evaluări
- Leung Et Al-2018-Clinical and Experimental OptometryDocument9 paginiLeung Et Al-2018-Clinical and Experimental Optometryangeles sanchez clariaÎncă nu există evaluări
- Tugas Baca OfkomDocument28 paginiTugas Baca OfkomGithasari DewiÎncă nu există evaluări
- Retinopathy of PrematurityDocument2 paginiRetinopathy of PrematurityCzarina Mae LomboyÎncă nu există evaluări
- 1Document2 pagini1Lady TerylleÎncă nu există evaluări
- Retinoblastoma - (Reh-Tin-Oh-BlastDocument18 paginiRetinoblastoma - (Reh-Tin-Oh-BlastRoi GamasÎncă nu există evaluări
- Year MSC Optometry Student) : University of Gondar Cmhs Departement of OptometryDocument63 paginiYear MSC Optometry Student) : University of Gondar Cmhs Departement of Optometryhaymanot aynalemÎncă nu există evaluări
- NotesDocument2 paginiNotesJasmin BonghanoyÎncă nu există evaluări
- Challenges RopDocument9 paginiChallenges RopdrtgodeÎncă nu există evaluări
- HyperopiaDocument6 paginiHyperopiageeneevzzÎncă nu există evaluări
- Retinitis Pigmentosa: Prepared By: Aditya SaxenaDocument17 paginiRetinitis Pigmentosa: Prepared By: Aditya Saxenaaditya0% (1)
- Jurnal MataDocument8 paginiJurnal MatamarinarizkiÎncă nu există evaluări
- Retinopathy of PrematurityDocument30 paginiRetinopathy of Prematuritykenikirkucing2Încă nu există evaluări
- Pediatric Glaucoma: Advice On Diagnosing and Managing A Rare But Potentially Devastating Group of DiseasesDocument4 paginiPediatric Glaucoma: Advice On Diagnosing and Managing A Rare But Potentially Devastating Group of DiseaseswidyastutiÎncă nu există evaluări
- Retinopathy of Prematurity UptodateDocument14 paginiRetinopathy of Prematurity UptodateSonia ChanÎncă nu există evaluări
- 14 F Crop CompleteDocument31 pagini14 F Crop CompleteManju ManjunathÎncă nu există evaluări
- Medical Case: Name: Rafie Lugassekti NIM: P1337430216038 Class: 1BDocument14 paginiMedical Case: Name: Rafie Lugassekti NIM: P1337430216038 Class: 1BRafieLugassektiÎncă nu există evaluări
- Biology Investigatory Project: Samiksha Subhashish SarkarDocument35 paginiBiology Investigatory Project: Samiksha Subhashish SarkarSamiksha SarkarÎncă nu există evaluări
- To Evaluate The Occurrence and To Analyse Risk Factors For The Development of ROP in A Tertiary Care HospitalDocument5 paginiTo Evaluate The Occurrence and To Analyse Risk Factors For The Development of ROP in A Tertiary Care HospitalInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Childhood BlindnessDocument6 paginiChildhood BlindnessMonika Diaz KristyanindaÎncă nu există evaluări
- Infantile Leukocoria The White Pupil PDFDocument4 paginiInfantile Leukocoria The White Pupil PDFDian HapsariÎncă nu există evaluări
- Retinopathy of Prematurity - HandoutDocument2 paginiRetinopathy of Prematurity - Handoutmusara87Încă nu există evaluări
- Anesthetic Concerns in Patients With Retinopathy of PrematurityDocument4 paginiAnesthetic Concerns in Patients With Retinopathy of Prematurityluizaradulescu4Încă nu există evaluări
- Myopia - EyeWikiDocument1 paginăMyopia - EyeWikiRima MaulinaÎncă nu există evaluări
- Approach To StrabismusDocument11 paginiApproach To StrabismusMuvenn KannanÎncă nu există evaluări
- Pediatr Clin Na 2014 Jun 61 (3) 495Document9 paginiPediatr Clin Na 2014 Jun 61 (3) 495mickymed_Încă nu există evaluări
- Glaucoma in Older Children: and AdolescentsDocument2 paginiGlaucoma in Older Children: and AdolescentsAnthonya KnightÎncă nu există evaluări
- Congenital Preventable Blindness: of ChildDocument4 paginiCongenital Preventable Blindness: of ChildJustin Michal DassÎncă nu există evaluări
- Ocular Disorders in The NewbornDocument11 paginiOcular Disorders in The NewbornXimena ParedesÎncă nu există evaluări
- 2013 PROF 220 AniridiaDocument5 pagini2013 PROF 220 Aniridiaavram_elenaÎncă nu există evaluări
- Prevalence and Progression of Myopia in Children at RaipurDocument9 paginiPrevalence and Progression of Myopia in Children at RaipurInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Glaucoma Note (DR - Abeba)Document17 paginiGlaucoma Note (DR - Abeba)creativejoburgÎncă nu există evaluări
- Intraocular Lenses and Clinical Treatment in Paediatric CataractDocument5 paginiIntraocular Lenses and Clinical Treatment in Paediatric CataractLinna LetoÎncă nu există evaluări
- Screening Examination of Premature Infants For Retinopathy of PrematurityDocument9 paginiScreening Examination of Premature Infants For Retinopathy of PrematurityArdhito BudhijuwonoÎncă nu există evaluări
- Congenital Cataract-Approach and Management ReviewDocument6 paginiCongenital Cataract-Approach and Management ReviewFirgietaPotterÎncă nu există evaluări
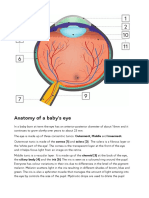
- Anatomy of A Baby's Eye: Outermost, Middle and Innermost. Cornea (1) and Sclera (2) - The Sclera Is A Fibrous Layer orDocument2 paginiAnatomy of A Baby's Eye: Outermost, Middle and Innermost. Cornea (1) and Sclera (2) - The Sclera Is A Fibrous Layer orSandor GyongyverÎncă nu există evaluări
- Student Handbook Orthoptics.Document13 paginiStudent Handbook Orthoptics.Nur AminÎncă nu există evaluări
- Lay Forum NotesDocument7 paginiLay Forum NotesCleoGomezÎncă nu există evaluări
- Myopia - Incidence, Pathogenesis, Management and New Possibilities of TreatmentDocument7 paginiMyopia - Incidence, Pathogenesis, Management and New Possibilities of TreatmenthanaddulÎncă nu există evaluări
- Congenital GlaucomaDocument27 paginiCongenital Glaucomaanon_373532435Încă nu există evaluări
- 2018.12.eye Conditions in Adults - Final 5th December 2018Document18 pagini2018.12.eye Conditions in Adults - Final 5th December 2018KOMATSU SHOVELÎncă nu există evaluări
- Update in ROP: Ophthalmology Department Andalas University/ DR M Djamil Hospital. PadangDocument33 paginiUpdate in ROP: Ophthalmology Department Andalas University/ DR M Djamil Hospital. PadangKemala SayutiÎncă nu există evaluări
- Literature Review On Refractive ErrorsDocument5 paginiLiterature Review On Refractive Errorsafmzfvlopbchbe100% (1)
- Macppt On Blindness by ArmaanDocument9 paginiMacppt On Blindness by ArmaanArmaandeep DhillonÎncă nu există evaluări
- Gejala LeukokoriaDocument37 paginiGejala LeukokoriaAnonymous mFKwUNÎncă nu există evaluări
- Eye Diseases: An Investigatory Project by Shrikanth Pillai XII BDocument11 paginiEye Diseases: An Investigatory Project by Shrikanth Pillai XII BCR7STUDIO 7100% (1)
- KELAINAN REFRAKSI NadiaDocument6 paginiKELAINAN REFRAKSI NadiaNadia A. DestiantiÎncă nu există evaluări
- Peri Operative Nursing ManagementDocument19 paginiPeri Operative Nursing ManagementSabina KontehÎncă nu există evaluări
- Joshua 24 15Document1 paginăJoshua 24 15api-313783690Încă nu există evaluări
- In The World of Nursing Education, The Nurs FPX 4900 Assessment Stands As A PivotalDocument3 paginiIn The World of Nursing Education, The Nurs FPX 4900 Assessment Stands As A Pivotalarthurella789Încă nu există evaluări
- Writing - Hidden Curriculum v2 EditedDocument6 paginiWriting - Hidden Curriculum v2 EditedwhighfilÎncă nu există evaluări
- Tugas Conditional Sentences YanneDocument3 paginiTugas Conditional Sentences Yanneyanne nurmalitaÎncă nu există evaluări
- Syllabus/Course Specifics - Fall 2009: TLT 480: Curricular Design and InnovationDocument12 paginiSyllabus/Course Specifics - Fall 2009: TLT 480: Curricular Design and InnovationJonel BarrugaÎncă nu există evaluări
- IBM System X UPS Guide v1.4.0Document71 paginiIBM System X UPS Guide v1.4.0Phil JonesÎncă nu există evaluări
- Approved Chemical ListDocument2 paginiApproved Chemical ListSyed Mansur Alyahya100% (1)
- Simulation of Channel Estimation and Equalization For WiMAX PHY Layer in Simulink PDFDocument6 paginiSimulation of Channel Estimation and Equalization For WiMAX PHY Layer in Simulink PDFayadmanÎncă nu există evaluări
- Is 13779 1999 PDFDocument46 paginiIs 13779 1999 PDFchandranmuthuswamyÎncă nu există evaluări
- Jesus Died: Summary: Jesus Died We Need To Have No Doubt About That. Without Jesus' Death We Would Have NoDocument6 paginiJesus Died: Summary: Jesus Died We Need To Have No Doubt About That. Without Jesus' Death We Would Have NoFabiano.pregador123 OliveiraÎncă nu există evaluări
- 2023-Tutorial 02Document6 pagini2023-Tutorial 02chyhyhyÎncă nu există evaluări
- Case Study 1 (Pneumonia)Document13 paginiCase Study 1 (Pneumonia)Kate EscotonÎncă nu există evaluări
- Need You Now Lyrics: Charles Scott, HillaryDocument3 paginiNeed You Now Lyrics: Charles Scott, HillaryAl UsadÎncă nu există evaluări
- Mezbah Uddin Ahmed (173-017-054) Chapter 11Document12 paginiMezbah Uddin Ahmed (173-017-054) Chapter 11riftÎncă nu există evaluări
- Re CrystallizationDocument25 paginiRe CrystallizationMarol CerdaÎncă nu există evaluări
- Thesis FulltextDocument281 paginiThesis FulltextEvgenia MakantasiÎncă nu există evaluări
- Feline Neonatal IsoerythrolysisDocument18 paginiFeline Neonatal IsoerythrolysisPaunas JoshiÎncă nu există evaluări
- Validator in JSFDocument5 paginiValidator in JSFvinh_kakaÎncă nu există evaluări
- Bfhi Poster A2Document1 paginăBfhi Poster A2api-423864945Încă nu există evaluări
- Business Finance and The SMEsDocument6 paginiBusiness Finance and The SMEstcandelarioÎncă nu există evaluări
- The Training Toolbox: Forced Reps - The Real Strength SenseiDocument7 paginiThe Training Toolbox: Forced Reps - The Real Strength SenseiSean DrewÎncă nu există evaluări
- Best-First SearchDocument2 paginiBest-First Searchgabby209Încă nu există evaluări
- Windows SCADA Disturbance Capture: User's GuideDocument23 paginiWindows SCADA Disturbance Capture: User's GuideANDREA LILIANA BAUTISTA ACEVEDOÎncă nu există evaluări