S-ar putea să vă placă și
- Defining Characteristic S Nursing Diagnosis Scientific Analysis Plan of Care Nursing Interventions Rationale Subjective: Short Term: IndependentDocument1 paginăDefining Characteristic S Nursing Diagnosis Scientific Analysis Plan of Care Nursing Interventions Rationale Subjective: Short Term: Independentboomer SeargeÎncă nu există evaluări
- A Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsDe la EverandA Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsÎncă nu există evaluări
- Drug StudyDocument5 paginiDrug StudyGAYOL BREEN IRAH A.Încă nu există evaluări
- Drug Study Pyrantel & CefuroximeDocument2 paginiDrug Study Pyrantel & CefuroximeMikhael Briones ApasÎncă nu există evaluări
- Heart Valve DiseaseDocument9 paginiHeart Valve DiseaseChaturangaNSenerathÎncă nu există evaluări
- NCPDocument8 paginiNCPFaustino LicudÎncă nu există evaluări
- Cardiovascular Agents ReviewerDocument18 paginiCardiovascular Agents ReviewerJoycel CeñidozaÎncă nu există evaluări
- MCN Introduction :physiologic Changes in Pregnancy..Document14 paginiMCN Introduction :physiologic Changes in Pregnancy..janet_alexisÎncă nu există evaluări
- Physical Examination and Review of Systems: Peri-Orbital Hematoma Sub-Conjunctiva Hemorrhage On Left EyeDocument3 paginiPhysical Examination and Review of Systems: Peri-Orbital Hematoma Sub-Conjunctiva Hemorrhage On Left EyeBianx Flores DosdosÎncă nu există evaluări
- CASE PRESentationDocument30 paginiCASE PRESentationllanelli.graciaÎncă nu există evaluări
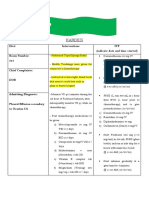
- Kardex: Diet: Interventions IVF (Indicate Date and Time Started) Room Number: 313Document2 paginiKardex: Diet: Interventions IVF (Indicate Date and Time Started) Room Number: 313kuro hanabusaÎncă nu există evaluări
- RevalidaDocument5 paginiRevalidaHawkins FletcherÎncă nu există evaluări
- Medication Administration Knowledge AssessmentDocument4 paginiMedication Administration Knowledge AssessmentkateÎncă nu există evaluări
- A Case Presentation - PediaDocument50 paginiA Case Presentation - PediaCathy ChiongÎncă nu există evaluări
- Potassium Chloride Injection: Product MonographDocument18 paginiPotassium Chloride Injection: Product MonographMatthew ParsonsÎncă nu există evaluări
- Nursing Physical AssessmentDocument5 paginiNursing Physical AssessmentApril Louise PaluganÎncă nu există evaluări
- CHFDocument35 paginiCHFNurayunie Abd HalimÎncă nu există evaluări
- Hypertension: Several Readings of High Blood Pressure, Thus Its Other NameDocument41 paginiHypertension: Several Readings of High Blood Pressure, Thus Its Other NameSophie Rose V R-zÎncă nu există evaluări
- Halamang Gamot TableDocument3 paginiHalamang Gamot TableReyo VillanuevaÎncă nu există evaluări
- Pernicious AnemiaDocument24 paginiPernicious AnemiaArthadian De PeraltaÎncă nu există evaluări
- Case in Herniorraphy BESTCASEDocument23 paginiCase in Herniorraphy BESTCASEAdrian MallarÎncă nu există evaluări
- Case Presentation (Final)Document35 paginiCase Presentation (Final)Denie BoyonasÎncă nu există evaluări
- Case Pres Ncps FinalDocument13 paginiCase Pres Ncps FinalMariejoy YadaoÎncă nu există evaluări
- UrethritisDocument11 paginiUrethritismarej143Încă nu există evaluări
- Case Study CvaDocument33 paginiCase Study CvaArmand Bong Santiago100% (1)
- Drug Study: Far Eastern UniversityDocument3 paginiDrug Study: Far Eastern UniversityChoy DacanayÎncă nu există evaluări
- Kawasaki DiseaseDocument7 paginiKawasaki DiseaseRitamariaÎncă nu există evaluări
- What Is Diphtheria?Document2 paginiWhat Is Diphtheria?Luna WhiteÎncă nu există evaluări
- Tetralogy of FallotDocument3 paginiTetralogy of FallotJohn Mark PocsidioÎncă nu există evaluări
- Filipino Culture, Values, and Practices in Relation To Difficult Childbearing and ChildrearingDocument8 paginiFilipino Culture, Values, and Practices in Relation To Difficult Childbearing and ChildrearingRheeanne AmilasanÎncă nu există evaluări
- FNCPDocument7 paginiFNCPMaria Ivy Rochelle TanÎncă nu există evaluări
- III. Symptomatology of CHFDocument9 paginiIII. Symptomatology of CHFMelanie GaledoÎncă nu există evaluări
- Case Scenario Osteoarthritis Week 16 GerontologDocument5 paginiCase Scenario Osteoarthritis Week 16 GerontologMary Josette NavarraÎncă nu există evaluări
- Pathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsDocument2 paginiPathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsAb Staholic Boii100% (1)
- Inv A Sion Pha Se: Bill Julius Samuel G. Alferez BSN IiiDocument1 paginăInv A Sion Pha Se: Bill Julius Samuel G. Alferez BSN IiiRudelsa Agcolicol LangamanÎncă nu există evaluări
- Zocor (Simvastatin)Document3 paginiZocor (Simvastatin)E100% (1)
- Far Eastern University: Institute of NursingDocument3 paginiFar Eastern University: Institute of Nursingshendae cosmianoÎncă nu există evaluări
- CHH Drug Study Week 3Document21 paginiCHH Drug Study Week 3maryxtine24Încă nu există evaluări
- H MoleDocument2 paginiH MoleJoanna Marie Datahan EstomoÎncă nu există evaluări
- Case Study PneumoniaDocument14 paginiCase Study PneumoniaJester GalayÎncă nu există evaluări
- THROMBOPHLEBITISDocument50 paginiTHROMBOPHLEBITISmers puno100% (3)
- Mechanism of HypertensionDocument4 paginiMechanism of HypertensionAlya Putri KhairaniÎncă nu există evaluări
- Path o Physiology of SyphilisDocument1 paginăPath o Physiology of Syphilis3S - JOCSON, DENESE NICOLE LEE M.Încă nu există evaluări
- Definition of PneumoniaDocument4 paginiDefinition of PneumoniaEmylia Ananda PutriÎncă nu există evaluări
- Pathophysiology On Fracture of Left Femoral Head: Precipitating Factor Predisposing FactorDocument2 paginiPathophysiology On Fracture of Left Femoral Head: Precipitating Factor Predisposing FactorEsther Mendez CatubigÎncă nu există evaluări
- Age - Weather: Aspiration of Secretions Containing MicrobesDocument4 paginiAge - Weather: Aspiration of Secretions Containing Microbeslouie john abilaÎncă nu există evaluări
- FNCP SampleDocument7 paginiFNCP SampleMarion Stacy LananteÎncă nu există evaluări
- Essential New Born Care ScriptDocument3 paginiEssential New Born Care ScriptShiela Joy DuquezÎncă nu există evaluări
- Pa Tho Physiology of RaDocument7 paginiPa Tho Physiology of Ralisalmar2008Încă nu există evaluări
- Case Study - Incomplete Abortion Related To APSDocument8 paginiCase Study - Incomplete Abortion Related To APSRomeo ReyesÎncă nu există evaluări
- Module 4 Nursing ProcessDocument14 paginiModule 4 Nursing ProcessArjay Cuh-ingÎncă nu există evaluări
- The Child With Hematologic DisordersDocument149 paginiThe Child With Hematologic DisordersNics FranciscoÎncă nu există evaluări
- Nursing Care Plan: Ineffective CopingDocument2 paginiNursing Care Plan: Ineffective CopingRosalinda SalvadorÎncă nu există evaluări
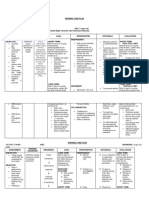
- Nursing Care Plan: Subjective: During 8 Hours Nursing Management: (5) After 8 HoursDocument4 paginiNursing Care Plan: Subjective: During 8 Hours Nursing Management: (5) After 8 HoursRawan KhateebÎncă nu există evaluări
- PneumoniaDocument4 paginiPneumoniaroscelle100% (1)
- ICS Pedia WardDocument8 paginiICS Pedia Wardsweet061991Încă nu există evaluări
- PATHOPHYSIO (Megaloblastic Anemia)Document3 paginiPATHOPHYSIO (Megaloblastic Anemia)Giselle EstoquiaÎncă nu există evaluări
- Angina Pectoris: Class Activity Evoking AnginaDocument4 paginiAngina Pectoris: Class Activity Evoking Anginamerin sunilÎncă nu există evaluări
- 2013 103 Notes 7Document18 pagini2013 103 Notes 7clarheenaÎncă nu există evaluări
- Appendectomy Case Presentation of JaysonDocument20 paginiAppendectomy Case Presentation of JaysonJaysonPangilinanAban100% (1)
- Informatic Solutions For Emergency Preparedness and ResponseDocument20 paginiInformatic Solutions For Emergency Preparedness and ResponseJaysonPangilinanAban100% (1)
- Acute Appendicitis PowerpointDocument34 paginiAcute Appendicitis PowerpointJaysonPangilinanAban100% (1)
- Upgrading Clinical Information SystemsDocument41 paginiUpgrading Clinical Information SystemsJaysonPangilinanAbanÎncă nu există evaluări
- Theories Frameworks and ModelsDocument33 paginiTheories Frameworks and ModelsJaysonPangilinanAbanÎncă nu există evaluări
- Ambulatory Care SystemDocument18 paginiAmbulatory Care SystemJaysonPangilinanAban100% (1)
- Internet Tools For Advance Nursing PracticeDocument4 paginiInternet Tools For Advance Nursing PracticeJaysonPangilinanAbanÎncă nu există evaluări
- Inevitable AbortionDocument21 paginiInevitable AbortionJaysonPangilinanAbanÎncă nu există evaluări
- Application in Nursing Informatics by TessDocument13 paginiApplication in Nursing Informatics by TessJaysonPangilinanAbanÎncă nu există evaluări
- Dependable Systems For Quality CareDocument14 paginiDependable Systems For Quality CareJaysonPangilinanAban100% (1)
- Electronic Health Records SystemDocument22 paginiElectronic Health Records SystemJaysonPangilinanAbanÎncă nu există evaluări
- NCP H-MoleDocument6 paginiNCP H-MoleJaysonPangilinanAban100% (3)
- UACE BIOLOGY PAPER 1 2005 Marking GuideDocument28 paginiUACE BIOLOGY PAPER 1 2005 Marking GuideKbale michealÎncă nu există evaluări
- Blood Circulatory SystemDocument5 paginiBlood Circulatory SystemAathifa ThowfeekÎncă nu există evaluări
- HIJAMA Ebook The Ultimate Cure For All Disease PDFDocument11 paginiHIJAMA Ebook The Ultimate Cure For All Disease PDFshaikhmuzu100% (4)
- BIOLOGYDocument5 paginiBIOLOGYDiana NurulÎncă nu există evaluări
- Frog Circulatory SystemDocument43 paginiFrog Circulatory Systembawcock100% (5)
- Anatomy of The Thorax MCQDocument7 paginiAnatomy of The Thorax MCQInnocent Clifford Marandu93% (14)
- Vascular DementiaDocument5 paginiVascular DementiaAna Ramos LopezÎncă nu există evaluări
- Introduction To Cardiac ElectrophysiologyDocument18 paginiIntroduction To Cardiac ElectrophysiologyNik-Othman C. Abdullah IIÎncă nu există evaluări
- 1 s2.0 S2666084923005089 MainDocument6 pagini1 s2.0 S2666084923005089 MainGabriel JoséÎncă nu există evaluări
- Auscultation of The HeartDocument84 paginiAuscultation of The HeartASTOASTOÎncă nu există evaluări
- WwerDocument2 paginiWwerMahdi AlattasÎncă nu există evaluări
- Ha Lec Session 14Document5 paginiHa Lec Session 14Klifford John RodriguezÎncă nu există evaluări
- Report Tetralogy of FallotDocument3 paginiReport Tetralogy of FallotLieana AguilarÎncă nu există evaluări
- Phase 1 Mixed (1) HusmDocument84 paginiPhase 1 Mixed (1) HusmSyed Shahrul Naz SyedÎncă nu există evaluări
- Medicine DamsDocument657 paginiMedicine DamsSubhashÎncă nu există evaluări
- JVP Examination For GPDocument43 paginiJVP Examination For GPYonathanHasudunganÎncă nu există evaluări
- Transcatheter Aortic Valve ImplantationDocument15 paginiTranscatheter Aortic Valve ImplantationJonathan BaileyÎncă nu există evaluări
- First Periodical Test g9Document7 paginiFirst Periodical Test g9lucia h. enriquezÎncă nu există evaluări
- NCP Ineffective Tissue PerfusionDocument4 paginiNCP Ineffective Tissue PerfusionSteffiÎncă nu există evaluări
- Hemodynamic Monitoring in Cardiogenic Shock: ReviewDocument6 paginiHemodynamic Monitoring in Cardiogenic Shock: ReviewLeyden Chavez VergaraÎncă nu există evaluări
- Cardiac Cycle: DR Nilesh Kate MBBS, MD Associate Prof Esic Medical College, Gulbarga. Dept. of PhysiologyDocument41 paginiCardiac Cycle: DR Nilesh Kate MBBS, MD Associate Prof Esic Medical College, Gulbarga. Dept. of Physiologyabdullah irpanÎncă nu există evaluări
- Emory Cardiology Newsletter June 2009Document9 paginiEmory Cardiology Newsletter June 2009hnaguÎncă nu există evaluări
- Molecules, Transport and HealthDocument29 paginiMolecules, Transport and Healthkamrunnisa100% (1)
- Discussion: 2.1 Tutorial DataDocument39 paginiDiscussion: 2.1 Tutorial DataTania Alsyabilla RuswandiÎncă nu există evaluări
- A New Echocardiographic Window To Visualize The Mitral Valve Complex During Mitral Valve Repair For Functional Mitral RegurgitationDocument3 paginiA New Echocardiographic Window To Visualize The Mitral Valve Complex During Mitral Valve Repair For Functional Mitral Regurgitationricardo villaÎncă nu există evaluări
- MCQ Cardiac SurgeryDocument86 paginiMCQ Cardiac Surgerynarnorata100% (5)
- PLAB BlueprintDocument140 paginiPLAB BlueprintCraig StropkayÎncă nu există evaluări
- Heart MurmursDocument7 paginiHeart MurmursOffvb MednuÎncă nu există evaluări
- CURRICULUM-MAP 1st Quarter Science 9Document4 paginiCURRICULUM-MAP 1st Quarter Science 9maria ana rehmontessori100% (2)
- Tutorial Ke-2 GDS 2: Grup B11Document60 paginiTutorial Ke-2 GDS 2: Grup B1118-176 Varian Andrew HartonoÎncă nu există evaluări
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)De la EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Evaluare: 3 din 5 stele3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 4.5 din 5 stele4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesDe la EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesEvaluare: 4.5 din 5 stele4.5/5 (1412)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 4 din 5 stele4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4.5 din 5 stele4.5/5 (6)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDe la EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisEvaluare: 3.5 din 5 stele3.5/5 (2)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDe la EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeEvaluare: 4.5 din 5 stele4.5/5 (254)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceDe la EverandTo Explain the World: The Discovery of Modern ScienceEvaluare: 3.5 din 5 stele3.5/5 (51)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsDe la EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsEvaluare: 4.5 din 5 stele4.5/5 (39)
- The Marshmallow Test: Mastering Self-ControlDe la EverandThe Marshmallow Test: Mastering Self-ControlEvaluare: 4.5 din 5 stele4.5/5 (60)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingDe la EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingEvaluare: 4 din 5 stele4/5 (1138)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)