S-ar putea să vă placă și
- The Value of Ultrasound in Detecting PneumothoraxDocument2 paginiThe Value of Ultrasound in Detecting PneumothoraxTsamara YumnaÎncă nu există evaluări
- Emergency Drugs PDFDocument34 paginiEmergency Drugs PDFTsamara YumnaÎncă nu există evaluări
- Cholesterol MS RADocument6 paginiCholesterol MS RATsamara YumnaÎncă nu există evaluări
- Jurnal ForensikDocument4 paginiJurnal ForensikTsamara YumnaÎncă nu există evaluări
- Beberapa Metode StatistikDocument1 paginăBeberapa Metode StatistikTsamara YumnaÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Chatburn 2 PDFDocument4 paginiChatburn 2 PDFJesus PlanellesÎncă nu există evaluări
- Clinical Manifestations and Assessment of Respiratory Disease 5th Edition Jardins Test BankDocument9 paginiClinical Manifestations and Assessment of Respiratory Disease 5th Edition Jardins Test Banksarahpalmerotpdkjcwfq100% (26)
- Daftar Pustaka Asma Dan PpokDocument7 paginiDaftar Pustaka Asma Dan PpokJames McmillanÎncă nu există evaluări
- 1.e. Bronchiolitis Treatment & Management - Approach Considerations, Initial Management, Admission CriteriaDocument12 pagini1.e. Bronchiolitis Treatment & Management - Approach Considerations, Initial Management, Admission CriteriaDavid CraigÎncă nu există evaluări
- AsthmaDocument46 paginiAsthmaHafiz Muhammad AeymonÎncă nu există evaluări
- Hubungan Merokok Dengan Asma Pada Usia LanjutDocument20 paginiHubungan Merokok Dengan Asma Pada Usia LanjutPuput Indah PratiwiÎncă nu există evaluări
- Comparison of Drug-Induced Sleep Endoscopy Ver2Document34 paginiComparison of Drug-Induced Sleep Endoscopy Ver2thtklÎncă nu există evaluări
- HYPERBARICDocument16 paginiHYPERBARICJihad Elias ChahlaÎncă nu există evaluări
- D Physiology of RespirationDocument45 paginiD Physiology of RespirationValluri Mukesh100% (1)
- Pneumothorax: - Cme - Mohamed Siruhan Supervisor: Dr. IanDocument64 paginiPneumothorax: - Cme - Mohamed Siruhan Supervisor: Dr. Ianinterna MANADOÎncă nu există evaluări
- Asthma Lesson PlanDocument29 paginiAsthma Lesson PlanRabiu Hassan Musa86% (7)
- Nursing Care PlanDocument9 paginiNursing Care PlanRenea Joy ArruejoÎncă nu există evaluări
- 2.lung InfectionsDocument5 pagini2.lung InfectionsDaraÎncă nu există evaluări
- EmphysemaDocument29 paginiEmphysemaMisheel OrgilsaikhanÎncă nu există evaluări
- Acute Bronchitis - StatPearls - NCBI BookshelfDocument7 paginiAcute Bronchitis - StatPearls - NCBI BookshelfnurulishtimalÎncă nu există evaluări
- Decanulasi TrakeostomiDocument6 paginiDecanulasi TrakeostomiDhiel Muhammad FarreyraÎncă nu există evaluări
- Anesthetic Management of Non-Fasted Patients Requiring Emergency SurgeryDocument17 paginiAnesthetic Management of Non-Fasted Patients Requiring Emergency SurgeryBhi-An BatobalonosÎncă nu există evaluări
- COPD NEW GuidelinesDocument45 paginiCOPD NEW GuidelinesMuhammad HaneefÎncă nu există evaluări
- Jurnal Bronchitis Dengan AsmaDocument5 paginiJurnal Bronchitis Dengan AsmaMauLan SaputraÎncă nu există evaluări
- TaniaDocument14 paginiTaniaOm SharmaÎncă nu există evaluări
- Spirometry Report Group-14Document11 paginiSpirometry Report Group-14Mwanja MosesÎncă nu există evaluări
- Asthma by ConsensusDocument87 paginiAsthma by ConsensusSatnam KaurÎncă nu există evaluări
- Asthma and Other Respiratory Medications DefindDocument4 paginiAsthma and Other Respiratory Medications DefindKiran ManojÎncă nu există evaluări
- Novilyn C. Pataray BSN - Ii Acute Epiglottis: St. Paul College of Ilocos SurDocument1 paginăNovilyn C. Pataray BSN - Ii Acute Epiglottis: St. Paul College of Ilocos SurCharina AubreyÎncă nu există evaluări
- Nursing Care Plan For Pneumonia NCPDocument3 paginiNursing Care Plan For Pneumonia NCPFARAH MAE MEDINAÎncă nu există evaluări
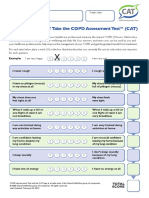
- How Is Your Copd? Take The Copd Assessmenttest (Cat) : Your Name: Today'S DateDocument1 paginăHow Is Your Copd? Take The Copd Assessmenttest (Cat) : Your Name: Today'S DateAndreea BurceaÎncă nu există evaluări
- Chest Trauma and Diseases: Mexigin Gayatri Akash JohannaDocument80 paginiChest Trauma and Diseases: Mexigin Gayatri Akash JohannadidiÎncă nu există evaluări
- Reasons For Testing: Air LungsDocument12 paginiReasons For Testing: Air LungsNathyÎncă nu există evaluări
- Respiratory Emergencies in ChildrenDocument66 paginiRespiratory Emergencies in Childrenlordoftheweb100% (7)
- Alveolar Stress How To Measure 2161 105X 1000273Document3 paginiAlveolar Stress How To Measure 2161 105X 1000273Ade Satria ElismanÎncă nu există evaluări