S-ar putea să vă placă și
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
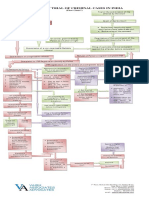
- Process of Trial of Criminal Cases in India (Flow Chart)Document1 paginăProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- 2019 - List of Equipment, Tools & MaterialsDocument3 pagini2019 - List of Equipment, Tools & Materialsreynald manzanoÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Marketing Communication I Assignment (Advertisement)Document13 paginiMarketing Communication I Assignment (Advertisement)Serene_98Încă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- By John Chaffee: Thinking CriticallyDocument6 paginiBy John Chaffee: Thinking CriticallygeoedukoreaÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- ECAT STD 2 Sample Question PaperDocument7 paginiECAT STD 2 Sample Question PaperVinay Jindal0% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- 20 Đề thi thử tốt nghiệp THPT năm 2021 - có đáp ánDocument131 pagini20 Đề thi thử tốt nghiệp THPT năm 2021 - có đáp ánThanh NganÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- I Am A Filipino by Carlos RomuloDocument7 paginiI Am A Filipino by Carlos RomuloKimberly NgÎncă nu există evaluări
- Fashion Designer Research Paper ThesisDocument4 paginiFashion Designer Research Paper Thesisafbteyrma100% (2)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Mindfulness of Breathing and The Four Elements MeditationDocument98 paginiMindfulness of Breathing and The Four Elements Meditationulrich_ehrenbergerÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Personal Details: Your Application Form Has Been Submitted Successfully. Payment Is SuccessfulDocument6 paginiPersonal Details: Your Application Form Has Been Submitted Successfully. Payment Is SuccessfulKanchanÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Wolfgang Tillmans - NoticeDocument74 paginiWolfgang Tillmans - NoticeSusana Vilas-BoasÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- El Poder de La Disciplina El Hábito Que Cambiará Tu Vida (Raimon Samsó)Document4 paginiEl Poder de La Disciplina El Hábito Que Cambiará Tu Vida (Raimon Samsó)ER CaballeroÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Case Study 1 - Whirlpool Reverser Logistics - With New Rubric - Winter 2022Document4 paginiCase Study 1 - Whirlpool Reverser Logistics - With New Rubric - Winter 2022ShravanÎncă nu există evaluări
- Xeljanz Initiation ChecklistDocument8 paginiXeljanz Initiation ChecklistRawan ZayedÎncă nu există evaluări
- Policy ScheduleDocument1 paginăPolicy ScheduleDinesh nawaleÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Articles of IncorporationDocument2 paginiArticles of IncorporationLegal Forms100% (1)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Flore Bridoux CV Sep 2016 Short VersionDocument10 paginiFlore Bridoux CV Sep 2016 Short Versionbayu_pancaÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Attachment 1 - Memorandum Order No. 21-1095 - Revised Guidelines For The Implementation of Shared Service Facilities (SSF) ProjectDocument28 paginiAttachment 1 - Memorandum Order No. 21-1095 - Revised Guidelines For The Implementation of Shared Service Facilities (SSF) ProjectMark Jurilla100% (1)
- Assignment 1684490923Document16 paginiAssignment 1684490923neha.engg45755Încă nu există evaluări
- Ind Nifty ItDocument2 paginiInd Nifty ItRaghavendraÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Knock Knock GamesDocument1 paginăKnock Knock GamesArsyta AnandaÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1091)
- Mobile DevGuide 13 - Gulde For Mobile DeveloperDocument258 paginiMobile DevGuide 13 - Gulde For Mobile DevelopersmaliscribdÎncă nu există evaluări
- CIR vs. Estate of Benigno P. Toda, JRDocument13 paginiCIR vs. Estate of Benigno P. Toda, JRMrln VloriaÎncă nu există evaluări
- Using Open-Ended Tools in Facilitating Mathematics and Science LearningDocument59 paginiUsing Open-Ended Tools in Facilitating Mathematics and Science LearningDomina Jayne PagapulaanÎncă nu există evaluări
- Basketball Coaching ToolboxDocument71 paginiBasketball Coaching Toolboxmensrea0Încă nu există evaluări
- Finals Lesson Ii Technology As A WAY of Revealing: Submitted By: Teejay M. AndrdaDocument8 paginiFinals Lesson Ii Technology As A WAY of Revealing: Submitted By: Teejay M. AndrdaTeejay AndradaÎncă nu există evaluări
- Theory of Design 2Document98 paginiTheory of Design 2Thirumeni MadavanÎncă nu există evaluări
- HTTP WWW - Aphref.aph - Gov.au House Committee Haa Overseasdoctors Subs Sub133Document3 paginiHTTP WWW - Aphref.aph - Gov.au House Committee Haa Overseasdoctors Subs Sub133hadia duraniÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- browningsong 안동Document68 paginibrowningsong 안동yooÎncă nu există evaluări
- Mass Effect 1 WalkthroughDocument143 paginiMass Effect 1 Walkthroughandyt10Încă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)