S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Art Martin and Janes Landrell - Neuro KinesiologyDocument91 paginiArt Martin and Janes Landrell - Neuro KinesiologySharon Anyosa Medina100% (2)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Chinese Magic: KuDocument30 paginiChinese Magic: KuDmitry Galtsin100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Parasities That HealthDocument48 paginiParasities That Healthtito19593Încă nu există evaluări
- 13-Secrets - Napoleon HillDocument14 pagini13-Secrets - Napoleon HillGastoreÎncă nu există evaluări
- 13-Secrets - Napoleon HillDocument14 pagini13-Secrets - Napoleon HillGastoreÎncă nu există evaluări
- D8045-16 Standard Test Method For Acid Number of Crude Oils and Petroleum Products by CatalyticDocument6 paginiD8045-16 Standard Test Method For Acid Number of Crude Oils and Petroleum Products by CatalytichishamÎncă nu există evaluări
- ENT Head and Neck ExamDocument21 paginiENT Head and Neck ExamvickyÎncă nu există evaluări
- Grade Control For Australian Open Pit Gold MinesDocument14 paginiGrade Control For Australian Open Pit Gold Mineswaldo100% (1)
- Pancreatic EnzymesDocument15 paginiPancreatic Enzymestito19593100% (3)
- Cocktail Making Techniques 13.3.11Document3 paginiCocktail Making Techniques 13.3.11Ryan MenezesÎncă nu există evaluări
- 9 Taoist Books On The ElixirDocument44 pagini9 Taoist Books On The Elixirtito19593100% (2)
- 9 Taoist Books On The ElixirDocument44 pagini9 Taoist Books On The Elixirtito19593100% (2)
- 06 - Flexible Operation of Thermal Power Plants - OEM Perspective and Experiences PDFDocument22 pagini06 - Flexible Operation of Thermal Power Plants - OEM Perspective and Experiences PDFRavishankarÎncă nu există evaluări
- Plum Blossom DivinationDocument1 paginăPlum Blossom Divinationtito19593100% (2)
- Charles de Harlez The Yih King 16pDocument30 paginiCharles de Harlez The Yih King 16ptito19593100% (1)
- MeiHua Divination Part 10Document27 paginiMeiHua Divination Part 10tito19593100% (3)
- Lesson 3.3 Inside An AtomDocument42 paginiLesson 3.3 Inside An AtomReign CallosÎncă nu există evaluări
- Soil ExplorationDocument42 paginiSoil ExplorationDilipKumarAkkaladevi100% (1)
- Supplementary Spec To API Specification 17D Subsea Wellhead and Tree Equipment With Justifications S 561Jv2022 11Document81 paginiSupplementary Spec To API Specification 17D Subsea Wellhead and Tree Equipment With Justifications S 561Jv2022 11maximusala83Încă nu există evaluări
- ISOM News 26.2Document4 paginiISOM News 26.2tito19593Încă nu există evaluări
- I Ching by JhianDocument10 paginiI Ching by JhianAna IrinaÎncă nu există evaluări
- Felipe 0001Document2 paginiFelipe 0001tito19593Încă nu există evaluări
- ISOM News 30.1Document10 paginiISOM News 30.1tito19593Încă nu există evaluări
- ISOM News 26.1 PDFDocument2 paginiISOM News 26.1 PDFtito19593Încă nu există evaluări
- Abordajes Terapéuticos en El Dolor Lumbar Crónico PDFDocument4 paginiAbordajes Terapéuticos en El Dolor Lumbar Crónico PDFtito19593Încă nu există evaluări
- ANTONIO MARTIN Effect of Fruits Vegetables or Vitamin E Rich DietDocument8 paginiANTONIO MARTIN Effect of Fruits Vegetables or Vitamin E Rich Diettito19593Încă nu există evaluări
- Andrew SaulDocument3 paginiAndrew Saultito19593Încă nu există evaluări
- ESP Tratado de Medicina Oculta y Magia PracticaDocument6 paginiESP Tratado de Medicina Oculta y Magia Practicatito195930% (1)
- DP201 User Manual (English) Lapiz OpticoDocument14 paginiDP201 User Manual (English) Lapiz Opticotito19593Încă nu există evaluări
- ESP Tratado de Medicina Oculta y Magia PracticaDocument6 paginiESP Tratado de Medicina Oculta y Magia Practicatito195930% (1)
- Bibliography CHINA 6PDocument17 paginiBibliography CHINA 6Ptito19593Încă nu există evaluări
- VSPlayer User Manual V6.2.0Document33 paginiVSPlayer User Manual V6.2.0klaucsÎncă nu există evaluări
- Russell Kirkland Dao de JingDocument10 paginiRussell Kirkland Dao de Jingtito19593Încă nu există evaluări
- Caras Conocidas Fisonomia MargaretDocument12 paginiCaras Conocidas Fisonomia Margarettito19593Încă nu există evaluări
- Calendario Lunar 1989eDocument1 paginăCalendario Lunar 1989etito19593Încă nu există evaluări
- Salvia para La CabezaDocument2 paginiSalvia para La Cabezatito19593Încă nu există evaluări
- TCM ZangfuDocument95 paginiTCM Zangfutito19593Încă nu există evaluări
- Convecc Ao Forc Ada Externa: Vicente Luiz ScalonDocument18 paginiConvecc Ao Forc Ada Externa: Vicente Luiz ScalonMaria VitóriaÎncă nu există evaluări
- Winchester Model 9422 Lever Action Rifle Owner's Manual: LicenseeDocument0 paginiWinchester Model 9422 Lever Action Rifle Owner's Manual: Licenseecarlosfanjul1Încă nu există evaluări
- Rotating Driver S Workstation and Rotating Cab: Reliable Solutions For More Ergonomic and Effective WorkingDocument12 paginiRotating Driver S Workstation and Rotating Cab: Reliable Solutions For More Ergonomic and Effective WorkingEduardo CapeletiÎncă nu există evaluări
- User Manual 4372070Document80 paginiUser Manual 4372070EDENILSON CORDEIROÎncă nu există evaluări
- PW6101 ProgrammationDocument44 paginiPW6101 ProgrammationCédric DekeyserÎncă nu există evaluări
- Main Group Oganometallics: Shriver and Atkins, Chapter 15Document24 paginiMain Group Oganometallics: Shriver and Atkins, Chapter 15José Augusto VillarÎncă nu există evaluări
- RBC Disorder BcqsDocument68 paginiRBC Disorder BcqsMukhtiar AhmedÎncă nu există evaluări
- SOP-M-003 Device Master Record Rev ADocument3 paginiSOP-M-003 Device Master Record Rev AAnil Chowadary Anil ChowadaryÎncă nu există evaluări
- Mechanism of Enzyme ActionDocument19 paginiMechanism of Enzyme ActionRubi AnnÎncă nu există evaluări
- BIS Ventilation Brochure enDocument16 paginiBIS Ventilation Brochure enBruno SantosÎncă nu există evaluări
- Static Fluid: It Is Mass Per Unit Volume at Certain TemperatureDocument11 paginiStatic Fluid: It Is Mass Per Unit Volume at Certain TemperatureMohamed El-GoharyÎncă nu există evaluări
- LaserDocument12 paginiLasercabe79Încă nu există evaluări
- Assessment 2 Vital Signs Normal ValuesDocument4 paginiAssessment 2 Vital Signs Normal Valuesthannikkotte12345Încă nu există evaluări
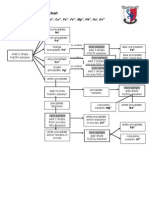
- Testing For Cations Flow ChartDocument2 paginiTesting For Cations Flow Chartapi-252561013Încă nu există evaluări
- Eastman Methyl N-Amyl Ketone (MAK) and Eastman Methyl Isoamyl Ketone (MIAK)Document4 paginiEastman Methyl N-Amyl Ketone (MAK) and Eastman Methyl Isoamyl Ketone (MIAK)Chemtools Chemtools100% (1)
- Subject: Invitation To Join As "Resource Speaker" On Our Seminar On Fire Prevention and Safety ConsciousnessDocument6 paginiSubject: Invitation To Join As "Resource Speaker" On Our Seminar On Fire Prevention and Safety ConsciousnessRjay CadaÎncă nu există evaluări
- Magicad Heating&Piping and Ventilation Version 2011.11: User'S GuideDocument285 paginiMagicad Heating&Piping and Ventilation Version 2011.11: User'S GuideCalin CalinÎncă nu există evaluări
- Fosroc Conplast SP335: Multi-Range Water Reducing AdmixtureDocument2 paginiFosroc Conplast SP335: Multi-Range Water Reducing AdmixtureVincent JavateÎncă nu există evaluări
- Single Conductor 15KV, Shielded, MV-105Document2 paginiSingle Conductor 15KV, Shielded, MV-105henry hernandezÎncă nu există evaluări
- Full Download Book Microbiome Immunity Digestive Health and Nutrition Epidemiology Pathophysiology Prevention and Treatment PDFDocument41 paginiFull Download Book Microbiome Immunity Digestive Health and Nutrition Epidemiology Pathophysiology Prevention and Treatment PDFmildred.walker324100% (15)
- Artifact 7 - Superannuation Pension Calculator-GuidelinesDocument2 paginiArtifact 7 - Superannuation Pension Calculator-GuidelinesSai RamÎncă nu există evaluări
- Machine Design II: Prof. K.Gopinath & Prof. M.M.MayuramDocument4 paginiMachine Design II: Prof. K.Gopinath & Prof. M.M.Mayurampredrag10Încă nu există evaluări