Dysmenorrhea refers to pain that is related to menstruation. ICD-10 N94.4N94.6.
There are two types of dysmenorrhea, primary and secondary.
Primary dysmenorrhea does not involve evidence of pelvis disease.
Secondary dysmenorrhea is associated with a disease such as pelvic inflammatory
disease. Typical pain is caused by contractions that are induced
by prostaglandins from the endometrium. As stated by Neinstein, Gordon, Katzman,
Rosen & Woods, 2009, p. 460, "Dysmenorrhea is the greatest single cause of lost
work and school hours in females, with >140 million hours lost per year".
For a patient that is experiencing dysmenorrhea, a history and physical would be
completed as well as possible lab work. When obtaining a history from an
adolescent, it is important that they are asked about the degree of pain they
experience during menstruation as well as if the pain interferes with their activities
of daily living and daily routines. Their previous use of pain relieving methods
should be obtained with the effectiveness of each. Anyone that may be sexually
active should be asked about any history of sexually transmitted diseases. Upon
the physical assessment, a complete review of systems will be conducted as well.
With dysmenorrhea, local symptoms include spasmodic pain in the lower abdomen
that may radiate to the back and thighs, nausea, fatigue, mood changes and
headache.
Differential diagnosis: Gynecologic causes can include pelvic inflammatory
disease, endometriosis and other anatomic abnormalities. Nongynecologic causes
can include gastrointestinal disorders, genitourinary abnormalties and
gastrointestinal disorders such as irritable bowel syndrome.
"Many teenagers with severe cramps suffer for years before they seek treatment
because they think painful periods are just part of growing up" (Sayre, 2008).
The two most effective treatments of dysmenorrhea are nonsteriodal antiinflammatory medications and oral contraceptives. It is said that approximately
80% of individuals pain is relieved by nonsteroidal anti-inflammatories and
approximately 90% of individuals pain is controlled with oral contraceptives.
Non pharmacologic therapies can include exercise and heat application.
If evaluation of the patient shows that there is no nongynecological cause of the
symptoms and treatment of the pain is not successful, then the patient may be
considered for further testing such as laprascopy.
S-ar putea să vă placă și
- Horses in Nursing HomesDocument3 paginiHorses in Nursing HomesWidfdsafdsaÎncă nu există evaluări
- MR Spock FIND THATDocument2 paginiMR Spock FIND THATWidfdsafdsaÎncă nu există evaluări
- MR Spock GEORGIADocument2 paginiMR Spock GEORGIAWidfdsafdsaÎncă nu există evaluări
- Dogs Fly ColombiaDocument2 paginiDogs Fly ColombiaWidfdsafdsaÎncă nu există evaluări
- MR Spock TUNJADocument2 paginiMR Spock TUNJAWidfdsafdsaÎncă nu există evaluări
- New Jersey ColombiaDocument4 paginiNew Jersey ColombiaWidfdsafdsaÎncă nu există evaluări
- MR Spock BOGOTADocument2 paginiMR Spock BOGOTAWidfdsafdsaÎncă nu există evaluări
- MR Spock TUNJA CALIDocument2 paginiMR Spock TUNJA CALIWidfdsafdsaÎncă nu există evaluări
- MR Spock TUNJA BOGOTADocument2 paginiMR Spock TUNJA BOGOTAWidfdsafdsaÎncă nu există evaluări
- MR Spock FLORIDADocument2 paginiMR Spock FLORIDAWidfdsafdsaÎncă nu există evaluări
- Mr. Spock's Connection to New Jersey Revealed in Search ResultsDocument2 paginiMr. Spock's Connection to New Jersey Revealed in Search ResultsWidfdsafdsaÎncă nu există evaluări
- MR Spock New YorkDocument2 paginiMR Spock New YorkWidfdsafdsaÎncă nu există evaluări
- NJ NY Dogs Swim Across Hudson RiverDocument3 paginiNJ NY Dogs Swim Across Hudson RiverWidfdsafdsaÎncă nu există evaluări
- Flying Dogs to BogotaDocument2 paginiFlying Dogs to BogotaWidfdsafdsaÎncă nu există evaluări
- RBC Medicine HatDocument3 paginiRBC Medicine HatWidfdsafdsaÎncă nu există evaluări
- About 2,550,000 Results (0.49 Seconds) : Colombia Colombia ColombiaDocument3 paginiAbout 2,550,000 Results (0.49 Seconds) : Colombia Colombia ColombiaWidfdsafdsaÎncă nu există evaluări
- About 2,450,000 Results (0.40 Seconds) : Medicine HatDocument3 paginiAbout 2,450,000 Results (0.40 Seconds) : Medicine HatWidfdsafdsaÎncă nu există evaluări
- Physical Examination Is ImportantDocument2 paginiPhysical Examination Is ImportantWidfdsafdsaÎncă nu există evaluări
- WBC Medicine HatDocument3 paginiWBC Medicine HatWidfdsafdsaÎncă nu există evaluări
- People Also Ask: Understanding Blood Tests For Dogs - Countryside Veterinary ..Document4 paginiPeople Also Ask: Understanding Blood Tests For Dogs - Countryside Veterinary ..WidfdsafdsaÎncă nu există evaluări
- Dogs of NigeriaDocument4 paginiDogs of NigeriaWidfdsafdsaÎncă nu există evaluări
- What a CBC Reveals About Your Cat's HealthDocument3 paginiWhat a CBC Reveals About Your Cat's HealthWidfdsafdsaÎncă nu există evaluări
- Dogs of ColombiaDocument4 paginiDogs of ColombiaWidfdsafdsaÎncă nu există evaluări
- People Also Ask: Sunday, April 24, 2022 (GMT+2) Time in Madrid, SpainDocument3 paginiPeople Also Ask: Sunday, April 24, 2022 (GMT+2) Time in Madrid, SpainWidfdsafdsaÎncă nu există evaluări
- Paypal Stock BuyDocument3 paginiPaypal Stock BuyWidfdsafdsaÎncă nu există evaluări
- Testosterone For Dogs: People Also AskDocument2 paginiTestosterone For Dogs: People Also AskWidfdsafdsaÎncă nu există evaluări
- People Also Ask: World Is Not YoursDocument3 paginiPeople Also Ask: World Is Not YoursWidfdsafdsaÎncă nu există evaluări
- SELL OR HOLDDocument4 paginiSELL OR HOLDWidfdsafdsaÎncă nu există evaluări
- Dogs Are Cool ColombiaDocument3 paginiDogs Are Cool ColombiaWidfdsafdsaÎncă nu există evaluări
- Nursing DocumentationDocument3 paginiNursing DocumentationWidfdsafdsaÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Test Bank Dental Management of The Medically Compromised Patient 9th Edition LittleDocument4 paginiTest Bank Dental Management of The Medically Compromised Patient 9th Edition LittleFit ragnerÎncă nu există evaluări
- Mayo Clinic BPPVDocument4 paginiMayo Clinic BPPVCS NarayananÎncă nu există evaluări
- Sas 40Document2 paginiSas 40Sistine Rose LabajoÎncă nu există evaluări
- Carolyn R. Zalameda-Castro, MDDocument9 paginiCarolyn R. Zalameda-Castro, MDeza floresÎncă nu există evaluări
- Child India March 2021Document35 paginiChild India March 2021suheena.CÎncă nu există evaluări
- Importance of Shat Kriyakala in Disease Diagnosis and ManagementDocument6 paginiImportance of Shat Kriyakala in Disease Diagnosis and ManagementSHUBHAM RAOÎncă nu există evaluări
- Coronavirus Grado 10 - 11 Primera ClaseDocument17 paginiCoronavirus Grado 10 - 11 Primera ClaseMARIO ANDRES BedoyaÎncă nu există evaluări
- ABCs of Neuroimaging - Ali YIKILMAZDocument45 paginiABCs of Neuroimaging - Ali YIKILMAZRanintha SurbaktiÎncă nu există evaluări
- Splenic Injuries PDFDocument2 paginiSplenic Injuries PDFdessy pradessyaÎncă nu există evaluări
- CANINE-Spontaneous Pneumothorax in DogsDocument7 paginiCANINE-Spontaneous Pneumothorax in Dogstaner_soysurenÎncă nu există evaluări
- Gloves, gown, mask, eye protection as needed based on anticipated exposureDocument46 paginiGloves, gown, mask, eye protection as needed based on anticipated exposureJayrelle D. SafranÎncă nu există evaluări
- A. Abnormal Blood Pressure Changes On ExerciseDocument1 paginăA. Abnormal Blood Pressure Changes On ExerciseosamahihiÎncă nu există evaluări
- Alopecia: By. Mr. P. Dhilip KumarDocument9 paginiAlopecia: By. Mr. P. Dhilip Kumarpreet kaur100% (1)
- General Pathology Practical Exam Renal PathologyDocument16 paginiGeneral Pathology Practical Exam Renal PathologyCherry RahimaÎncă nu există evaluări
- Biostatistic and Epidemiology Lecture NoteDocument66 paginiBiostatistic and Epidemiology Lecture Notefff100% (3)
- Neonatal Sepsis, Opthalmia Neonatarum & HIV/AIDSDocument15 paginiNeonatal Sepsis, Opthalmia Neonatarum & HIV/AIDSSAKSHI RANAÎncă nu există evaluări
- Vaccines in Zimbabwe InformationDocument8 paginiVaccines in Zimbabwe InformationIsaac GumboÎncă nu există evaluări
- Miscellaneous Viruses: An Overview of Rubella, Parvo, HPV, Rotavirus and Other Gastrointestinal VirusesDocument7 paginiMiscellaneous Viruses: An Overview of Rubella, Parvo, HPV, Rotavirus and Other Gastrointestinal VirusesskÎncă nu există evaluări
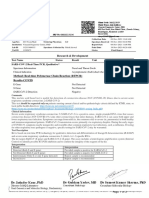
- Research & Development: Test Name Status Result Unit Reference Interval SARS-COV-2 Real-Time PCR, QualitativeDocument2 paginiResearch & Development: Test Name Status Result Unit Reference Interval SARS-COV-2 Real-Time PCR, QualitativeakashÎncă nu există evaluări
- Performance Task in Empowerment Technologies (Arthur King v. Leaño III, 11-Ipil (ABM-MODULAR)Document13 paginiPerformance Task in Empowerment Technologies (Arthur King v. Leaño III, 11-Ipil (ABM-MODULAR)Mary AuxileÎncă nu există evaluări
- Washington Secretary of Health Order 20-03: Statewide Face CoveringsDocument4 paginiWashington Secretary of Health Order 20-03: Statewide Face CoveringsKING 5 NewsÎncă nu există evaluări
- Dr. Muhammad Bilal Shah: Historical Evolution of EpidemiologyDocument36 paginiDr. Muhammad Bilal Shah: Historical Evolution of EpidemiologymuhammadbilalshahÎncă nu există evaluări
- Fever enDocument2 paginiFever enAbraham TheodoreÎncă nu există evaluări
- Computer-Based English Proficiency Test AdvisoryDocument7 paginiComputer-Based English Proficiency Test AdvisoryJoyce CarilloÎncă nu există evaluări
- Pengaruh Hipertensi Terhadap Kejadian Penyakit Jaringan Periodontal (Periodontitis) Pada Masyarakat Indonesia (Data Riskesdas 2018)Document8 paginiPengaruh Hipertensi Terhadap Kejadian Penyakit Jaringan Periodontal (Periodontitis) Pada Masyarakat Indonesia (Data Riskesdas 2018)Brili AnenoÎncă nu există evaluări
- A Complicated Case of Incisional HerniaDocument29 paginiA Complicated Case of Incisional Herniabheemrajy00Încă nu există evaluări
- GCSE Biology - Health and Disease - WorksheetDocument2 paginiGCSE Biology - Health and Disease - WorksheetVeenaÎncă nu există evaluări
- Guideline MERS Management in Malaysia, 2023Document123 paginiGuideline MERS Management in Malaysia, 2023Nezly IderusÎncă nu există evaluări
- Lifestyle, Genetics and Environment Predispose to DiseaseDocument4 paginiLifestyle, Genetics and Environment Predispose to DiseaseJohnnette BedoniaÎncă nu există evaluări
- Pressure UlcersDocument43 paginiPressure UlcersZubda Butt100% (2)