S-ar putea să vă placă și
- National Health SituationDocument23 paginiNational Health SituationKen HelmuthÎncă nu există evaluări
- Health Care Delivery System Lecture Handout PDFDocument9 paginiHealth Care Delivery System Lecture Handout PDFelle bello100% (1)
- 2 Community Healtyh Nursing - Field in NursingDocument12 pagini2 Community Healtyh Nursing - Field in NursingsannsannÎncă nu există evaluări
- The Present Status of Doh Immunization Program in Igorot CommunityDocument20 paginiThe Present Status of Doh Immunization Program in Igorot Communitymr. nicart50% (2)
- CHN MODULE 2 For StudentsDocument8 paginiCHN MODULE 2 For StudentsJoshua MendozaÎncă nu există evaluări
- MHGAP Philippines PDFDocument44 paginiMHGAP Philippines PDFLe Oj C PascuaÎncă nu există evaluări
- Maternal, Newborn and Child Health and Nutrition Strategy (Manual of Operations)Document235 paginiMaternal, Newborn and Child Health and Nutrition Strategy (Manual of Operations)Misyel AvelinoÎncă nu există evaluări
- Doh Health ProgramsDocument21 paginiDoh Health Programsrgng_1880304050% (2)
- Community Phc2 RleDocument12 paginiCommunity Phc2 Rleefermin_lovely100% (1)
- The Philippine Health AgendaDocument32 paginiThe Philippine Health Agendajustbeingclever100% (2)
- The Health Care Delivery SystemDocument114 paginiThe Health Care Delivery SystemBea Bianca CruzÎncă nu există evaluări
- Ethico-Legal Considerations in The Care of Older AdultDocument25 paginiEthico-Legal Considerations in The Care of Older AdultMarlone James OcenaÎncă nu există evaluări
- Philippine Health Care Delivery SystemDocument2 paginiPhilippine Health Care Delivery Systemhana_kimi498270Încă nu există evaluări
- Public Health Nursing 8X13Document11 paginiPublic Health Nursing 8X13RUIZ JAKE CANCILLER. VELARDEÎncă nu există evaluări
- DOH Programs A-ZDocument4 paginiDOH Programs A-ZFleur Jenne100% (1)
- Expanded Program On ImmunizationDocument13 paginiExpanded Program On Immunizationrceponelas1127Încă nu există evaluări
- Copar ProposalDocument3 paginiCopar ProposalJoy Mariel Isadora BurgosÎncă nu există evaluări
- Overview of Devolution of Health Services in The PhilippinesDocument5 paginiOverview of Devolution of Health Services in The PhilippinesAPIDSRU Surveillance100% (1)
- Expanded Program On ImmunizationDocument45 paginiExpanded Program On ImmunizationRuby Corazon Ediza100% (3)
- MCN National HealthDocument4 paginiMCN National HealthCamille RamosÎncă nu există evaluări
- CO and COPAR Notes For SendingDocument19 paginiCO and COPAR Notes For SendingMikko McDonie VeloriaÎncă nu există evaluări
- FHSISDocument31 paginiFHSISNezer SorianoÎncă nu există evaluări
- ABC's Food PreparationDocument11 paginiABC's Food Preparationann camposÎncă nu există evaluări
- Philippine Health Care SystemDocument72 paginiPhilippine Health Care Systemmarvinbreyes67% (9)
- Community DiagnosisDocument27 paginiCommunity DiagnosisSree Visakh100% (3)
- DOH ProgramsDocument114 paginiDOH ProgramsAlyssandra Luceno100% (6)
- Philippine Health Care System 2008Document72 paginiPhilippine Health Care System 2008api-385605192% (25)
- 2F Community Health Nursing Process NotesDocument11 pagini2F Community Health Nursing Process NotesCAUSIN, Lance Matthew,Încă nu există evaluări
- Urban Health System DevelopmentDocument7 paginiUrban Health System DevelopmentGlayza Pelle TiuÎncă nu există evaluări
- NCM 104 Lecture Chapter 1 BSN 2CDocument82 paginiNCM 104 Lecture Chapter 1 BSN 2CWilma Nierva BeraldeÎncă nu există evaluări
- Mandatory Infants and Children Health Immunization Act of 2011 Compulsory ImmunizationDocument3 paginiMandatory Infants and Children Health Immunization Act of 2011 Compulsory Immunizationbunso padilla100% (2)
- PHC Phcds DohDocument11 paginiPHC Phcds DohHet rodÎncă nu există evaluări
- Nursing Process in The Care of Population Groups and CommunityDocument6 paginiNursing Process in The Care of Population Groups and CommunitySamantha Bernardo UndaÎncă nu există evaluări
- Integrated Helminth Control Program (IHCP) : Date VenueDocument31 paginiIntegrated Helminth Control Program (IHCP) : Date VenueAnonymous100% (2)
- AO 2008-0029 Rapid Reduction of Maternal and Neonatal MortalityDocument13 paginiAO 2008-0029 Rapid Reduction of Maternal and Neonatal MortalitygiogmailÎncă nu există evaluări
- Primary Health Care 2 1232967837997879 3Document42 paginiPrimary Health Care 2 1232967837997879 3JL CalvinÎncă nu există evaluări
- 10 Doh Programs: Prepared By: Dhonnalyn A. Caballero, RNDocument28 pagini10 Doh Programs: Prepared By: Dhonnalyn A. Caballero, RNAnne Geleen BariasÎncă nu există evaluări
- Project NARSDocument3 paginiProject NARSRovefrances ErpeluaÎncă nu există evaluări
- The Health Promotion HandbookDocument63 paginiThe Health Promotion HandbookOnyd Subingsubing100% (1)
- Health Care Delivery SystemDocument40 paginiHealth Care Delivery SystemjosephÎncă nu există evaluări
- Micronutrient Program - Department of HealthDocument3 paginiMicronutrient Program - Department of HealthMelvin MarzanÎncă nu există evaluări
- MDG CHNDocument12 paginiMDG CHNMarie Joyce Faith RelucioÎncă nu există evaluări
- The Nursing Process in The Care of The CommunityDocument96 paginiThe Nursing Process in The Care of The CommunityCzarina Aeri RollorataÎncă nu există evaluări
- Reaction On The The Philippine Health Agenda 2016Document5 paginiReaction On The The Philippine Health Agenda 2016Jesselle Iquin100% (3)
- Ilem - Dispelling Myths, Correcting Misconceptions in Family PlanningDocument21 paginiIlem - Dispelling Myths, Correcting Misconceptions in Family PlanningaishiellcastilloÎncă nu există evaluări
- Fatima Community Diagnosis ToolDocument5 paginiFatima Community Diagnosis Toolkrisfred14100% (2)
- COPARDocument48 paginiCOPARJasmin Jacob100% (2)
- Framework For Maternal and Child Health NursingDocument26 paginiFramework For Maternal and Child Health NursingLeo Santos Magno75% (4)
- Community OrganizationDocument8 paginiCommunity OrganizationJon EricÎncă nu există evaluări
- Primary Health Care (PHC) in The PhilDocument23 paginiPrimary Health Care (PHC) in The PhilCLAUDETTE ANNE CORMARY100% (3)
- Nurse EntrepreneurshipDocument3 paginiNurse EntrepreneurshipWendy EscalanteÎncă nu există evaluări
- FOURmula OneDocument15 paginiFOURmula Onejona phie Montero100% (1)
- CHN 2 1-7 Formative Quiz #2B - NCM 113 - Community Health Nursing Ii - Population Groups andDocument5 paginiCHN 2 1-7 Formative Quiz #2B - NCM 113 - Community Health Nursing Ii - Population Groups andRegine CuntapayÎncă nu există evaluări
- O Define The Type of Nursing Service Provided o Listing The Criteria For Admission, EnrollmentDocument13 paginiO Define The Type of Nursing Service Provided o Listing The Criteria For Admission, EnrollmentKasandra Dawn Moquia BerisoÎncă nu există evaluări
- CHN Written Report (Devolution of Health Services)Document2 paginiCHN Written Report (Devolution of Health Services)Marco BaltazarÎncă nu există evaluări
- Breastfeeding HospitalDocument37 paginiBreastfeeding Hospitalemmanjabasa100% (1)
- Entrepre NurseDocument14 paginiEntrepre NurseWendy EscalanteÎncă nu există evaluări
- Philippine Health AgendaDocument11 paginiPhilippine Health Agenda2226205Încă nu există evaluări
- The Philippine Health Agenda 2016 To 2022 PDFDocument11 paginiThe Philippine Health Agenda 2016 To 2022 PDFmuncadamonicaÎncă nu există evaluări
- GLOBALDocument10 paginiGLOBALTiffany AdriasÎncă nu există evaluări
- Camp APOLLO Batch 8 - PC Mastercamp WorksheetDocument276 paginiCamp APOLLO Batch 8 - PC Mastercamp WorksheetSheryl AlapadÎncă nu există evaluări
- Do Not Delay A4Document1 paginăDo Not Delay A4Sheryl AlapadÎncă nu există evaluări
- TFG Tips On Creating A Good ResumeDocument3 paginiTFG Tips On Creating A Good ResumeSheryl AlapadÎncă nu există evaluări
- Summary of Benefits: Life Your TermDocument1 paginăSummary of Benefits: Life Your TermSheryl AlapadÎncă nu există evaluări
- The Absolute Divorce Act of 2018Document18 paginiThe Absolute Divorce Act of 2018Sheryl AlapadÎncă nu există evaluări
- Christmas in The Philippine Pasko Sa Aming Bayang Pilipinas: TH THDocument14 paginiChristmas in The Philippine Pasko Sa Aming Bayang Pilipinas: TH THSheryl AlapadÎncă nu există evaluări
- Absolute Divorce For PPT DraftDocument4 paginiAbsolute Divorce For PPT DraftSheryl AlapadÎncă nu există evaluări
- Mendiola Massacre Statement 2015Document3 paginiMendiola Massacre Statement 2015Sheryl Alapad100% (1)
- Ms. Eugene Domingo Actress Dear Ms. EugeneDocument1 paginăMs. Eugene Domingo Actress Dear Ms. EugeneSheryl AlapadÎncă nu există evaluări
- Land Reform in The Philippines Asian SurveyDocument26 paginiLand Reform in The Philippines Asian SurveySheryl AlapadÎncă nu există evaluări
- An Anarchy of Families State and Family in The PhilippinesDocument21 paginiAn Anarchy of Families State and Family in The PhilippinesSheryl AlapadÎncă nu există evaluări
- Rarejob Training Skill Assessment FAQsDocument28 paginiRarejob Training Skill Assessment FAQsSheryl Alapad100% (1)
- Bioethics Session 9 SASDocument7 paginiBioethics Session 9 SASAnthony BadiliÎncă nu există evaluări
- Reference Tracking Sheet - From June 2018 V1Document313 paginiReference Tracking Sheet - From June 2018 V1Calum SyersÎncă nu există evaluări
- Quiz: How Much Do You Know About Universal Health CoverageDocument2 paginiQuiz: How Much Do You Know About Universal Health CoverageAlina DanielaÎncă nu există evaluări
- What Is Free Health CareDocument2 paginiWhat Is Free Health CareTaimoor HassanÎncă nu există evaluări
- Costing Exercise Report - Vietnam Primary CareDocument9 paginiCosting Exercise Report - Vietnam Primary CareRémi DANHOUNDOÎncă nu există evaluări
- Health Care Models: International Comparisons: Dr. Jaime Llambías-Wolff, Ph.D. York UniversityDocument22 paginiHealth Care Models: International Comparisons: Dr. Jaime Llambías-Wolff, Ph.D. York UniversityTas SafetyTradeÎncă nu există evaluări
- Philhealth: Romeo R. Andaya, MD - MSCPD, PHD, Fpafp Chair, DPMCHDocument19 paginiPhilhealth: Romeo R. Andaya, MD - MSCPD, PHD, Fpafp Chair, DPMCHKatÎncă nu există evaluări
- PH Case Study - iHEA - FinalDocument8 paginiPH Case Study - iHEA - FinalMaria Eufemia C YapÎncă nu există evaluări
- Annotated Bibliography Draft-1Document5 paginiAnnotated Bibliography Draft-1api-217663549Încă nu există evaluări
- Alexis Rogers - Imi Pono ApplicationDocument2 paginiAlexis Rogers - Imi Pono Applicationapi-482292533Încă nu există evaluări
- The Health and Care System Explained - GOV - UKDocument5 paginiThe Health and Care System Explained - GOV - UKkaidÎncă nu există evaluări
- Planning Commission Report On Universal Health CoveragaDocument343 paginiPlanning Commission Report On Universal Health Coveragasethirupal2001Încă nu există evaluări
- Module 1 - Framework of Maternal and Child Health Nursing 2023Document12 paginiModule 1 - Framework of Maternal and Child Health Nursing 2023AinaB ManaloÎncă nu există evaluări
- dm2022 0530Document4 paginidm2022 0530Meme LangÎncă nu există evaluări
- FICCI EY Report Healthcare ReportDocument72 paginiFICCI EY Report Healthcare Reportsh_niravÎncă nu există evaluări
- WeHnMa1 - CA0l Agenda AandB CWC Puri 2 PDFDocument320 paginiWeHnMa1 - CA0l Agenda AandB CWC Puri 2 PDFRavi SrivastavaÎncă nu există evaluări
- Advantages and Disadvantages of Free HealthcareDocument1 paginăAdvantages and Disadvantages of Free HealthcareJames DayritÎncă nu există evaluări
- A Comprehensive Health Labour Market Framework For Universal Health CoverageDocument3 paginiA Comprehensive Health Labour Market Framework For Universal Health Coveragecwag68Încă nu există evaluări
- Thailand'S Universal Health Coverage: Dr. Thaworn Sakunphanit MD., FRCPT, Ba (Econ), Msc. (Social Policy Financing)Document17 paginiThailand'S Universal Health Coverage: Dr. Thaworn Sakunphanit MD., FRCPT, Ba (Econ), Msc. (Social Policy Financing)IManÎncă nu există evaluări
- Health Systems Strengthening, Universal Health Coverage, Health Security and ResilienceDocument1 paginăHealth Systems Strengthening, Universal Health Coverage, Health Security and ResilienceCharles ChalimbaÎncă nu există evaluări
- Reviewer in CHNN (Rle) : "Bag Technique"Document31 paginiReviewer in CHNN (Rle) : "Bag Technique"Claudine Jo B. Talaboc100% (1)
- 13 125450Document2 pagini13 125450Anonymous ryRmzUIEvÎncă nu există evaluări
- Nhif Attachment ReportDocument18 paginiNhif Attachment ReportHãmsïk Då Mâjór Ëñ-jéçtõr100% (3)
- Feasibility Assessment and Financial Projection Results For A Social Health Insurance Scheme in SwazilandDocument96 paginiFeasibility Assessment and Financial Projection Results For A Social Health Insurance Scheme in SwazilandbejarhasanÎncă nu există evaluări
- Universal Health Care in The Philippines - From Policy To PracticeDocument216 paginiUniversal Health Care in The Philippines - From Policy To PracticeLloyd Leonell LabsoÎncă nu există evaluări
- Philippine Health Care Delivery SystemDocument10 paginiPhilippine Health Care Delivery SystemKristel AnneÎncă nu există evaluări
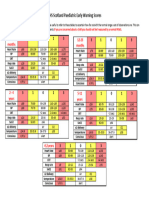
- GP Poster - Pews Tables FinalDocument1 paginăGP Poster - Pews Tables Finalanitn2020Încă nu există evaluări
- Drug Reimbursement Regulation in 6 Peer CountriesDocument8 paginiDrug Reimbursement Regulation in 6 Peer CountriessunnyÎncă nu există evaluări
- Kenya Health Financing Strategy - FinalDocument85 paginiKenya Health Financing Strategy - Finalwhoosh2008Încă nu există evaluări
- Factors Affecting CHF Enrollment in TanzaniaDocument56 paginiFactors Affecting CHF Enrollment in TanzaniacharlesÎncă nu există evaluări