S-ar putea să vă placă și
- The Acupuncture Prescription:: A Holistic Approach to HealthDe la EverandThe Acupuncture Prescription:: A Holistic Approach to HealthÎncă nu există evaluări
- Five Phase Treatments DR ManakaDocument20 paginiFive Phase Treatments DR ManakaKoa Carlos CastroÎncă nu există evaluări
- Fourflowers PDFDocument4 paginiFourflowers PDFPedro Lagos Marques NetoÎncă nu există evaluări
- Acupuncture Pulse Diagnosis and the Constitutional Conditional ParadigmDe la EverandAcupuncture Pulse Diagnosis and the Constitutional Conditional ParadigmÎncă nu există evaluări
- Prostate Problems Giovani Masciocia PDFDocument8 paginiProstate Problems Giovani Masciocia PDFarielighÎncă nu există evaluări
- Stop Suffering from Arthritis: Tcm Can Help YouDe la EverandStop Suffering from Arthritis: Tcm Can Help YouÎncă nu există evaluări
- TCM Student Study GuideDocument40 paginiTCM Student Study GuideHomework PingÎncă nu există evaluări
- Immortalizing Emotions: A Chinese Medicine perspective of TattoosDe la EverandImmortalizing Emotions: A Chinese Medicine perspective of TattoosÎncă nu există evaluări
- 2008 Acupuncture Core Therapy - ToCDocument15 pagini2008 Acupuncture Core Therapy - ToCdoktormin106100% (1)
- Earth Persona: Mnemonic Method an Informal Chinese Herbal GuidebookDe la EverandEarth Persona: Mnemonic Method an Informal Chinese Herbal GuidebookÎncă nu există evaluări
- Shang Han LunDocument7 paginiShang Han LunJohanna Birriel SalcedoÎncă nu există evaluări
- Formulas That Regulate Qi & Blood: HBR Class 11Document58 paginiFormulas That Regulate Qi & Blood: HBR Class 11keiraku100% (2)
- Physical Examination in Cardiovascular Chinese MedicineDe la EverandPhysical Examination in Cardiovascular Chinese MedicineÎncă nu există evaluări
- Pulsynergy Made Easy, Part II: Leading Acupuncture CE ProviderDocument41 paginiPulsynergy Made Easy, Part II: Leading Acupuncture CE ProviderOmar BaÎncă nu există evaluări
- Sa-Ahm Five Element Acupuncture PDFDocument12 paginiSa-Ahm Five Element Acupuncture PDFlashmiÎncă nu există evaluări
- New Paradigms for Shang Han Lun - Integrating Korean Sasang Constitutional Medicine and Japanese Kampo MedicineDe la EverandNew Paradigms for Shang Han Lun - Integrating Korean Sasang Constitutional Medicine and Japanese Kampo MedicineÎncă nu există evaluări
- The Three Basic Components of A Pulse: Shape, Jump, and LevelDocument3 paginiThe Three Basic Components of A Pulse: Shape, Jump, and LevelShahul Hameed100% (1)
- On the Theory and Practical Application of Channels and CollateralsDe la EverandOn the Theory and Practical Application of Channels and CollateralsÎncă nu există evaluări
- Shang Han Lun OverviewDocument3 paginiShang Han Lun OverviewPedro Maia80% (5)
- Diabetes Perspectives and TreatmentsDocument32 paginiDiabetes Perspectives and TreatmentsyellahfellahÎncă nu există evaluări
- Wei SyndromeDocument8 paginiWei SyndromeezraallenÎncă nu există evaluări
- TCM DiagnosisDocument7 paginiTCM DiagnosisravenadlerÎncă nu există evaluări
- Comprehensive Index to Find Musculoskeletal ConditionsDocument16 paginiComprehensive Index to Find Musculoskeletal ConditionsMustafa Ali0% (1)
- The Eight Gua and Herbal FormulasDocument10 paginiThe Eight Gua and Herbal FormulasrendaoÎncă nu există evaluări
- Abdominal AcupunctureDocument2 paginiAbdominal Acupuncturetomas100% (2)
- Hmccann Hatung LN PDFDocument9 paginiHmccann Hatung LN PDFMiguel A Cordero100% (1)
- Pulse & Tongue LectureDocument6 paginiPulse & Tongue Lectureapi-26938624100% (3)
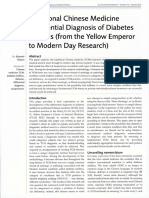
- TCM Diferential Dignosis of DM - Yellow EmperorDocument9 paginiTCM Diferential Dignosis of DM - Yellow EmperorLiliana PonteÎncă nu există evaluări
- Bodymapping Acupuncture Technique: in The Spirit of Master Tung - Cole Magbanua MacomDocument4 paginiBodymapping Acupuncture Technique: in The Spirit of Master Tung - Cole Magbanua Macomgefabifa0% (2)
- Pulsynergy Made Easy, Part III: by Dr. Jimmy Wei-Yen ChangDocument36 paginiPulsynergy Made Easy, Part III: by Dr. Jimmy Wei-Yen ChangOmar BaÎncă nu există evaluări
- Maciocia FormulasDocument4 paginiMaciocia FormulasMario RossiÎncă nu există evaluări
- TCM Principles of TreatmentDocument5 paginiTCM Principles of TreatmentJames O'SullivanÎncă nu există evaluări
- Needle Technique (Charles Chace)Document4 paginiNeedle Technique (Charles Chace)Tim SchlankÎncă nu există evaluări
- Cwang Tungfemale LN TCMWTDocument14 paginiCwang Tungfemale LN TCMWTdrprasant50% (2)
- Understanding Jing Fang Formula Patterns Through Case StudiesDocument3 paginiUnderstanding Jing Fang Formula Patterns Through Case StudiesMatthieu DecalfÎncă nu există evaluări
- Acupuncture As A FasciaDocument5 paginiAcupuncture As A Fasciacelliastt100% (1)
- The 29 Pulses in Chinese Medicine (TCM) Pulse DiagnosisDocument7 paginiThe 29 Pulses in Chinese Medicine (TCM) Pulse DiagnosisPrakash Aradhya RÎncă nu există evaluări
- Six Syndrom SystemDocument2 paginiSix Syndrom SystemDandhi Firmansyah100% (1)
- 2020 BIO Content Outline With Bibliography Jan 20Document12 pagini2020 BIO Content Outline With Bibliography Jan 20taoglider69020% (1)
- Special PointsDocument16 paginiSpecial Pointsshamsorah100% (4)
- School of Febrile Diseases History Development DiagnosisDocument9 paginiSchool of Febrile Diseases History Development DiagnosisJaffer Aftab0% (1)
- Chapter 6Document64 paginiChapter 6Jiayi100% (1)
- The Function of The PointsDocument175 paginiThe Function of The Pointsacuhome100% (2)
- Diabetes MellitusDocument8 paginiDiabetes Mellitusab21423Încă nu există evaluări
- 03-16 Jimmuy Pulse III FinalDocument3 pagini03-16 Jimmuy Pulse III FinalShahul HameedÎncă nu există evaluări
- GlaucomaDocument6 paginiGlaucomaratamanoÎncă nu există evaluări
- Tung Lower PointsDocument76 paginiTung Lower Pointscharanmann916550% (2)
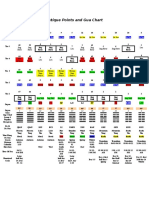
- Ancient Chinese Gua Chart and Organ PointsDocument1 paginăAncient Chinese Gua Chart and Organ PointsPedro MaiaÎncă nu există evaluări
- Shi Er Energy Meridians ChartDocument12 paginiShi Er Energy Meridians ChartSaša Balanesković100% (1)
- Herb Comps Review QuizletDocument6 paginiHerb Comps Review Quizletpeter911cmÎncă nu există evaluări
- DR Tans Acupuncture 1 2 3Document23 paginiDR Tans Acupuncture 1 2 3Omar Ba100% (1)
- Alchemical Facial Acupuncture Protocols, Part 3: by Mary Elizabeth Wakefield, Lac, Dipl. Ac., MS, MMDocument3 paginiAlchemical Facial Acupuncture Protocols, Part 3: by Mary Elizabeth Wakefield, Lac, Dipl. Ac., MS, MMHaryono zhuÎncă nu există evaluări
- Acupuncture 3-Points For AutismDocument3 paginiAcupuncture 3-Points For AutismHaryono zhu100% (1)
- Pattern Identification Acording To Qi BloodDocument7 paginiPattern Identification Acording To Qi BloodCarleta StanÎncă nu există evaluări
- Patterns of Disharmony BestDocument75 paginiPatterns of Disharmony Bestshamsorah100% (3)
- Convex-Shaped Pulses: by Jimmy Wei-Yen Chang, L.AcDocument3 paginiConvex-Shaped Pulses: by Jimmy Wei-Yen Chang, L.AcShahul HameedÎncă nu există evaluări
- Supporting Oncology Symptoms With TCM, Part IDocument98 paginiSupporting Oncology Symptoms With TCM, Part IWilliam TellÎncă nu există evaluări
- Essential Oil For Blood Sugar BalanceDocument18 paginiEssential Oil For Blood Sugar BalanceNevaeh Valli Deeva100% (2)
- Gentle Warriors Pediatric Formula GuideDocument80 paginiGentle Warriors Pediatric Formula Guidegiovanna2004100% (1)
- Travell and Simons' Myofascial Pain and Dysfunction (Vol 1) 2nd Ed - D. Simons, Et Al., (Williams and Wilkins, 1999) WWDocument1.052 paginiTravell and Simons' Myofascial Pain and Dysfunction (Vol 1) 2nd Ed - D. Simons, Et Al., (Williams and Wilkins, 1999) WWGeo Sanchez88% (34)
- A Comparison Between TCM and Dr. Tan's Balance Method PDFDocument46 paginiA Comparison Between TCM and Dr. Tan's Balance Method PDFCeline de Haan100% (6)
- A Comparison Between TCM and Dr. Tan's Balance Method PDFDocument46 paginiA Comparison Between TCM and Dr. Tan's Balance Method PDFCeline de Haan100% (6)
- Gentle Warriors Pediatric Formula GuideDocument80 paginiGentle Warriors Pediatric Formula Guidegiovanna2004100% (1)
- Gentle Warriors Pediatric Formula GuideDocument80 paginiGentle Warriors Pediatric Formula Guidegiovanna2004100% (1)
- Chinese Acupuncture TestsDocument257 paginiChinese Acupuncture TestsCeline de Haan100% (20)
- Chinese Acupuncture TestsDocument257 paginiChinese Acupuncture TestsCeline de Haan100% (20)
- Tong DiagnoseDocument1 paginăTong DiagnoseCeline de HaanÎncă nu există evaluări
- Chinese Acupuncture TestsDocument257 paginiChinese Acupuncture TestsCeline de Haan100% (20)
- Beef Farm Lab Report FinalDocument9 paginiBeef Farm Lab Report Finalapi-316728389100% (2)
- Acute AbdomenDocument16 paginiAcute AbdomenOnkar SinghÎncă nu există evaluări
- Full Speech by President Gotabaya Rajapaksa at "The Future of Asia" ConferenceDocument10 paginiFull Speech by President Gotabaya Rajapaksa at "The Future of Asia" ConferenceAdaderana OnlineÎncă nu există evaluări
- Chinese Remedy of Herbal Medicine To Treat H1N1 FluDocument2 paginiChinese Remedy of Herbal Medicine To Treat H1N1 FluCheng Bei HoneybeeÎncă nu există evaluări
- Gerald Crabtree - Trends in Genetics. Our Fragile IntellectDocument6 paginiGerald Crabtree - Trends in Genetics. Our Fragile IntellectDemocracia real YA100% (1)
- 1 - The Following Are Absorbable SuturesDocument15 pagini1 - The Following Are Absorbable SuturesKhaled ShaheenÎncă nu există evaluări
- Urban Health New DisciplineDocument2 paginiUrban Health New DisciplineJenny PinillaÎncă nu există evaluări
- Screening Brazilian Plants for Antimicrobial ActivityDocument5 paginiScreening Brazilian Plants for Antimicrobial ActivityDian Fitri ChairunnisaÎncă nu există evaluări
- Course Syllabus For Community Health Nursing and Communicable Disease NursingDocument2 paginiCourse Syllabus For Community Health Nursing and Communicable Disease NursingPhilippineNursingDirectory.com100% (15)
- IMNCI Chart Booklet (New) OrignalDocument36 paginiIMNCI Chart Booklet (New) OrignaleresdÎncă nu există evaluări
- Ultimate MJDF Part 1Document89 paginiUltimate MJDF Part 1SueChen Tan75% (4)
- Public Health 101 SeriesDocument58 paginiPublic Health 101 SeriesKiki Ari LarasÎncă nu există evaluări
- Post Operative DR MarshalDocument20 paginiPost Operative DR MarshalPrastia StratosÎncă nu există evaluări
- Breast AnatomyDocument53 paginiBreast AnatomyShriniwas RushiÎncă nu există evaluări
- Colloidal Silver - The Natural Antibiotic Alternative PDFDocument25 paginiColloidal Silver - The Natural Antibiotic Alternative PDFRobert Glen Murrell Jr100% (1)
- Antibiotic Susceptibility TestingDocument46 paginiAntibiotic Susceptibility Testingditta antÎncă nu există evaluări
- Evaluating PHC Services in CebuDocument34 paginiEvaluating PHC Services in CebuEricson MitraÎncă nu există evaluări
- Call For The Other Side of Justice By: Halima B. AbdulmaguidDocument1 paginăCall For The Other Side of Justice By: Halima B. AbdulmaguidRy FernandezÎncă nu există evaluări
- Tropical Sprue 2329 891X.1000130Document3 paginiTropical Sprue 2329 891X.1000130Grifanda HumairahÎncă nu există evaluări
- Know About Dengue FeverDocument11 paginiKnow About Dengue FeverKamlesh SanghaviÎncă nu există evaluări
- Legionella Awareness Presentation 1Document22 paginiLegionella Awareness Presentation 1Lan Tian50% (2)
- #Disease of External EarDocument4 pagini#Disease of External EarameerabestÎncă nu există evaluări
- General Hospital Psychiatry: SciencedirectDocument8 paginiGeneral Hospital Psychiatry: SciencedirectArgonne Robert AblanqueÎncă nu există evaluări
- The Dry EyeDocument8 paginiThe Dry EyeMohit BooraÎncă nu există evaluări
- English 8 - Summative TestDocument3 paginiEnglish 8 - Summative Testramel pastranoÎncă nu există evaluări
- Borang Mohon VisaDocument4 paginiBorang Mohon Visanadirah400Încă nu există evaluări
- Ventro FilDocument4 paginiVentro FilMichael DavisÎncă nu există evaluări
- Medical Asepsis TechniquesDocument6 paginiMedical Asepsis TechniquesChetan KumarÎncă nu există evaluări
- Rheumatoid ArthritisDocument25 paginiRheumatoid ArthritisGandung PrakosoÎncă nu există evaluări