S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Bone Marrow TransplantationDocument21 paginiBone Marrow TransplantationMorrison George100% (1)
- Management of Shock in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sceinces Kochi, KeralaDocument77 paginiManagement of Shock in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sceinces Kochi, KeralaAETCM Emergency medicineÎncă nu există evaluări
- Active Management of 3RD Stage of LaborDocument7 paginiActive Management of 3RD Stage of LaborFarheen khanÎncă nu există evaluări
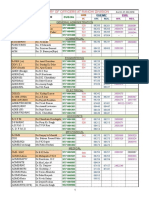
- CGHS Rates - Ranchi1Document110 paginiCGHS Rates - Ranchi1bug1lovebug2-1Încă nu există evaluări
- Consent FormsDocument111 paginiConsent Formsbug1lovebug2-1100% (1)
- 1540353267953-Telephone Directory Ranchi DivisionDocument3 pagini1540353267953-Telephone Directory Ranchi Divisionbug1lovebug2-1Încă nu există evaluări
- Precihole Sports Owner's Manual - NX100 PDFDocument12 paginiPrecihole Sports Owner's Manual - NX100 PDFbug1lovebug2-1Încă nu există evaluări
- Emergency MGT at HomeDocument15 paginiEmergency MGT at Homebug1lovebug2-1Încă nu există evaluări
- Exercise No 6 - On of Vitamin B Complex Skin TestingDocument2 paginiExercise No 6 - On of Vitamin B Complex Skin TestingpharmaebooksÎncă nu există evaluări
- AHPBA/SSO/SSAT Consensus Conference On Resectable and Borderline Resectable Pancreatic Cancer: Rationale and Overview of The ConferenceDocument2 paginiAHPBA/SSO/SSAT Consensus Conference On Resectable and Borderline Resectable Pancreatic Cancer: Rationale and Overview of The ConferenceGosadorÎncă nu există evaluări
- Fad Diet Research PaperDocument6 paginiFad Diet Research Papervehysad1s1w3100% (1)
- 2018 Refeeding Syndrome in The Frail Elderly PopulationDocument10 pagini2018 Refeeding Syndrome in The Frail Elderly PopulationManual de VacunaciónÎncă nu există evaluări
- Editorial For December 2010 - Rare RemediesDocument4 paginiEditorial For December 2010 - Rare Remediespanniyin selvanÎncă nu există evaluări
- Research Chapter 1 SampleDocument5 paginiResearch Chapter 1 Samplebea gÎncă nu există evaluări
- FastfoodDocument13 paginiFastfoodapi-488116516Încă nu există evaluări
- At The Crossroads of Lipid Metabolism and InflammationDocument7 paginiAt The Crossroads of Lipid Metabolism and InflammationChow Sing SingÎncă nu există evaluări
- THESIS of GROUP 2Document298 paginiTHESIS of GROUP 2renatoÎncă nu există evaluări
- Patricia Nicole Y.Cruz 2BSA-4 Module 2: Lesson 1-Assignment #1Document4 paginiPatricia Nicole Y.Cruz 2BSA-4 Module 2: Lesson 1-Assignment #1Patricia CruzÎncă nu există evaluări
- Gastro Graf inDocument12 paginiGastro Graf inquileuteÎncă nu există evaluări
- Dgca Module 09 Part 01Document11 paginiDgca Module 09 Part 01RAVI SHUKLAÎncă nu există evaluări
- Secdocument - 61download Breast Pathology 2Nd Edition David J Dabbs Full ChapterDocument67 paginiSecdocument - 61download Breast Pathology 2Nd Edition David J Dabbs Full Chapterjulia.swanson282100% (5)
- Golden Pearls of Gynecology and Obstetrics by DR Nadeem SHBDocument10 paginiGolden Pearls of Gynecology and Obstetrics by DR Nadeem SHBusamaÎncă nu există evaluări
- Biology Chapter 7Document3 paginiBiology Chapter 7JUDY100% (1)
- Glutathione FinalDocument33 paginiGlutathione Finalapi-103232543Încă nu există evaluări
- Periodontitis in Established Rheumatoid Arthritis Patients: A Cross-Sectional Clinical, Microbiological and Serological StudyDocument10 paginiPeriodontitis in Established Rheumatoid Arthritis Patients: A Cross-Sectional Clinical, Microbiological and Serological StudyalumeraÎncă nu există evaluări
- MRCP Part 1 (1)Document23 paginiMRCP Part 1 (1)ChloeÎncă nu există evaluări
- Sanna Labs PDFDocument4 paginiSanna Labs PDFmudassarhasan786Încă nu există evaluări
- Pictorial Review: Congenital Spine and Spinal Cord MalformationsDocument12 paginiPictorial Review: Congenital Spine and Spinal Cord MalformationsDr.Samreen SulthanaÎncă nu există evaluări
- Tinea Corporis An Updated ReviewDocument12 paginiTinea Corporis An Updated ReviewM Ilham FadillahÎncă nu există evaluări
- Eucalyptol Safety and Pharmacological ProfileDocument8 paginiEucalyptol Safety and Pharmacological ProfileTim ThomasÎncă nu există evaluări
- SSLC Model Question Paper 2022Document9 paginiSSLC Model Question Paper 2022AyazÎncă nu există evaluări
- Fart FileDocument3 paginiFart Fileanon_991097212Încă nu există evaluări
- Diabetes Mellitus Surgical PatientDocument33 paginiDiabetes Mellitus Surgical PatientGerald AndersonÎncă nu există evaluări
- FITT 2 (Midterm)Document13 paginiFITT 2 (Midterm)CJyn PascualÎncă nu există evaluări
- MRCPUK Part II Sample QuestionsDocument302 paginiMRCPUK Part II Sample QuestionsadiÎncă nu există evaluări